Hill L Drew, Edwards Rufus, Turner Jay R, Argo Yuma D, Olkhanud Purevdorj B, Odsuren Munkhtuul, Guttikunda Sarath, Ochir Chimedsuren, Smith Kirk R
Division of Environmental Health Sciences, University of California, Berkeley, CA, United States of America.
Department of Epidemiology, University of California Irvine, Irvine, CA, United States of America.
PLoS One. 2017 Oct 31;12(10):e0186834. doi: 10.1371/journal.pone.0186834. eCollection 2017.
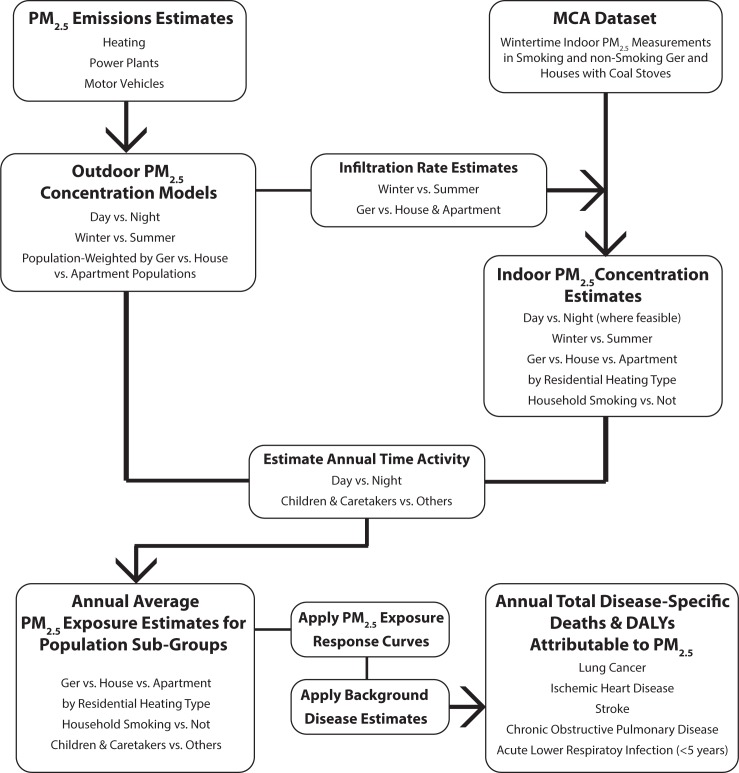
Winter air pollution in Ulaanbaatar, Mongolia is among the worst in the world. The health impacts of policy decisions affecting air pollution exposures in Ulaanbaatar were modeled and evaluated under business as usual and two more-strict alternative emissions pathways through 2024. Previous studies have relied on either outdoor or indoor concentrations to assesses the health risks of air pollution, but the burden is really a function of total exposure. This study combined projections of indoor and outdoor concentrations of PM2.5 with population time-activity estimates to develop trajectories of total age-specific PM2.5 exposure for the Ulaanbaatar population. Indoor PM2.5 contributions from secondhand tobacco smoke (SHS) were estimated in order to fill out total exposures, and changes in population and background disease were modeled. The health impacts were derived using integrated exposure-response curves from the Global Burden of Disease Study.
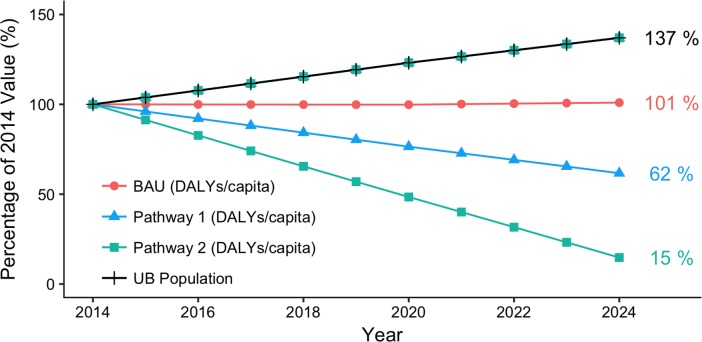
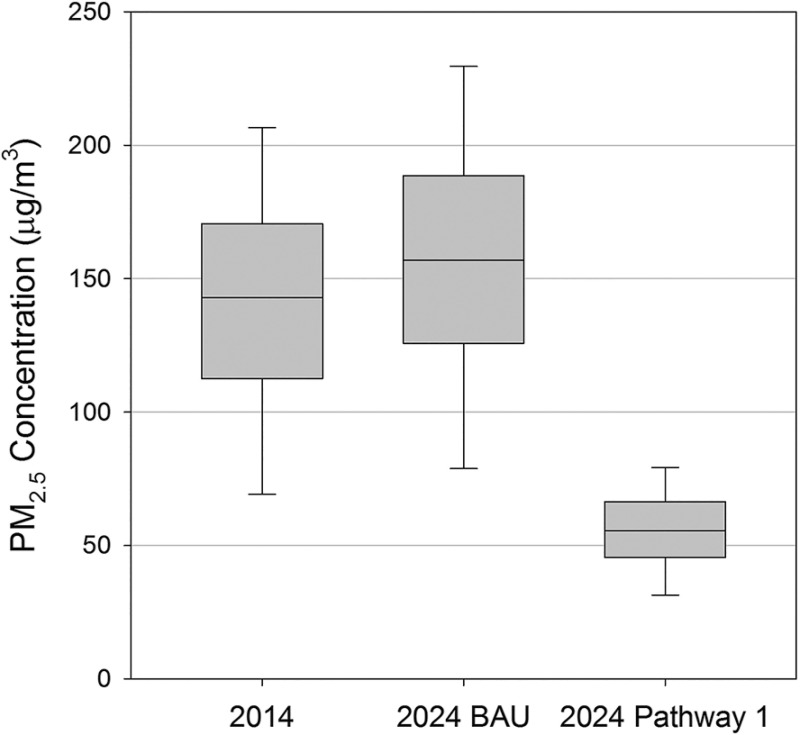
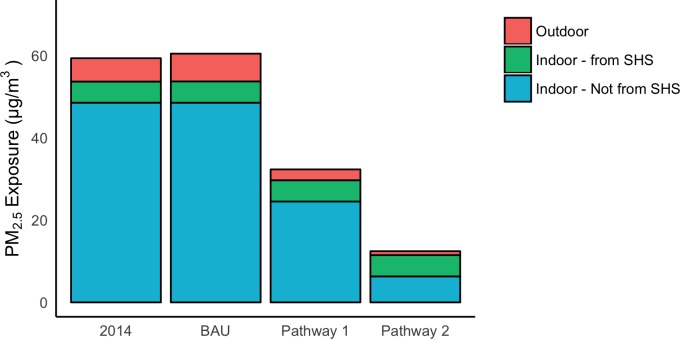
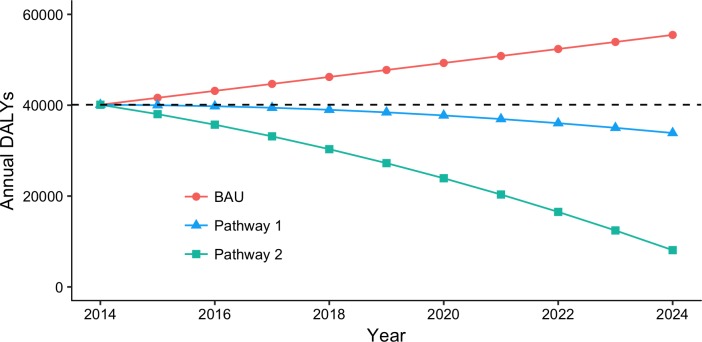
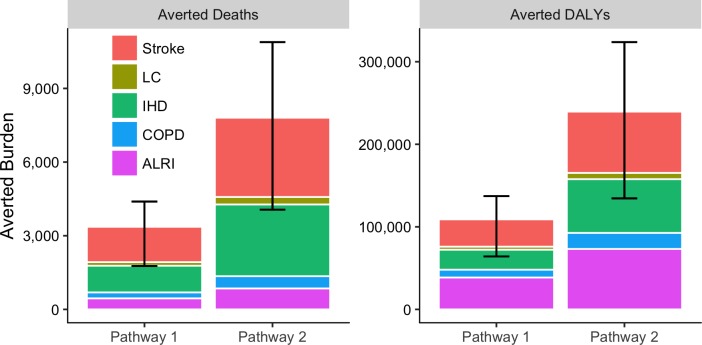
Annual average population-weighted PM2.5 exposures at baseline (2014) were estimated at 59 μg/m3. These were dominated by exposures occurring indoors, influenced considerably by infiltrated outdoor pollution. Under current control policies, exposures increased slightly to 60 μg/m3 by 2024; under moderate emissions reductions and under a switch to clean technologies, exposures were reduced from baseline levels by 45% and 80%, respectively. The moderate improvement pathway decreased per capita annual disability-adjusted life year (DALY) and death burdens by approximately 40%. A switch to clean fuels decreased per capita annual DALY and death burdens by about 85% by 2024 with the relative SHS contribution increasing substantially.
This study demonstrates a way to combine estimated changes in total exposure, background disease and population levels, and exposure-response functions to project the health impacts of alternative policy pathways. The resulting burden analysis highlights the need for aggressive action, including the elimination of residential coal burning and the reduction of current smoking rates.
蒙古乌兰巴托的冬季空气污染是世界上最严重的之一。对影响乌兰巴托空气污染暴露的政策决策的健康影响,在照常营业以及到2024年的另外两条更严格的替代排放路径下进行了建模和评估。以往的研究要么依靠室外浓度,要么依靠室内浓度来评估空气污染的健康风险,但负担实际上是总暴露的函数。本研究将PM2.5室内和室外浓度的预测与人口时间活动估计相结合,以制定乌兰巴托人口按年龄划分的PM2.5总暴露轨迹。估计了二手烟(SHS)对室内PM2.5的贡献,以完善总暴露情况,并对人口和背景疾病的变化进行了建模。使用全球疾病负担研究的综合暴露-反应曲线得出健康影响。
基线(2014年)时,年度平均人口加权PM2.5暴露估计为59μg/m³。这些暴露主要发生在室内,受到渗入的室外污染的显著影响。在当前的控制政策下,到2024年暴露量略有增加,达到60μg/m³;在适度减排和转向清洁技术的情况下,暴露量分别从基线水平降低了45%和80%。适度改善路径使人均年度残疾调整生命年(DALY)和死亡负担降低了约40%。到2024年,转向清洁燃料使人均年度DALY和死亡负担降低了约85%,二手烟的相对贡献大幅增加。
本研究展示了一种结合总暴露、背景疾病和人口水平的估计变化以及暴露-反应函数来预测替代政策路径的健康影响的方法。由此产生的负担分析突出了采取积极行动的必要性,包括消除居民燃煤和降低当前的吸烟率。