Sone Kazuki, Muramatsu Hideki, Nakao Makoto, Kagawa Yusuke, Kurokawa Ryota, Sato Hidefumi, Niimi Akio
Department of Respiratory Medicine, Kainan Hospital Aichi Prefectural Welfare Federation of Agricultural Cooperatives, Japan.
Department of Respiratory Medicine, Allergy and Clinical Immunology, Nagoya City University Graduate School of Medical Sciences, Japan.
Intern Med. 2018 Feb 1;57(3):383-386. doi: 10.2169/internalmedicine.8746-16. Epub 2017 Nov 1.
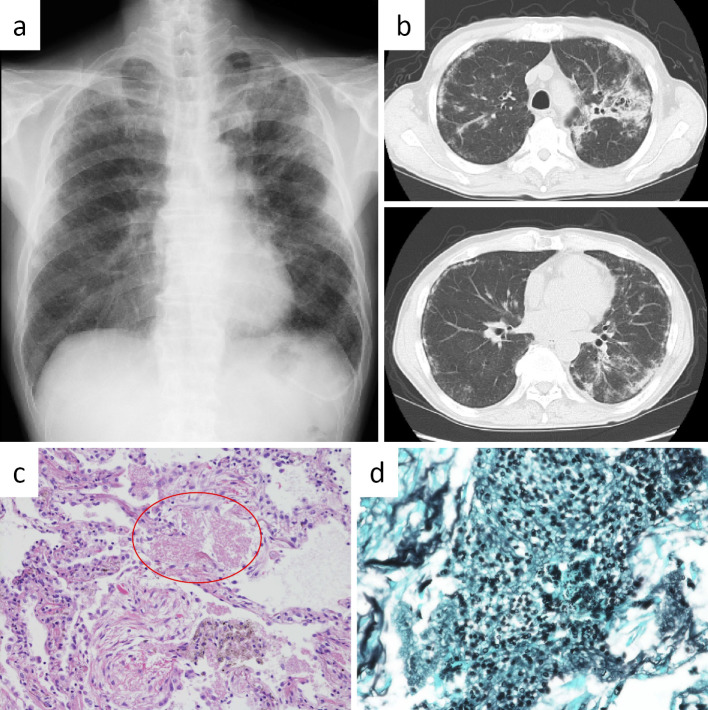
A 67-year-old man was admitted to our hospital complaining of dry cough. Chest computed tomography showed diffuse infiltrates and ground-glass opacities in the bilateral lung fields. Transbronchial lung biopsy specimens showed alveoli filled with yeast-like fungi. With a diagnosis of pneumocystis pneumonia (PCP), he was given oral sulfamethoxazole/trimethoprim, to which he responded well. However, seven months later, PCP relapsed. Analyses revealed a low bronchoalveolar lavage fluid CD4/CD8 ratio of 0.04 and CD4+ lymphocytopenia (250/μL). Despite intensive work-up, we were unable to detect the underlying cause of CD4+ lymphocytopenia; therefore, a final diagnosis of idiopathic CD4+ T-lymphocytopenia was made.
一名67岁男性因干咳入院。胸部计算机断层扫描显示双侧肺野弥漫性浸润和磨玻璃影。经支气管肺活检标本显示肺泡内充满酵母样真菌。诊断为肺孢子菌肺炎(PCP)后,给予口服磺胺甲恶唑/甲氧苄啶,治疗效果良好。然而,七个月后,PCP复发。分析显示支气管肺泡灌洗液CD4/CD8比值低至0.04,且存在CD4+淋巴细胞减少(250/μL)。尽管进行了全面检查,仍未能检测到CD4+淋巴细胞减少的潜在原因;因此,最终诊断为特发性CD4+ T淋巴细胞减少症。