Lanini Simone, Minosse Claudia, Vairo Francesco, Garbuglia Annarosa, Di Bari Virginia, Agresta Alessandro, Rezza Giovanni, Puro Vincenzo, Pendenza Alessio, Loffredo Maria Rosaria, Scognamiglio Paola, Zumla Alimuddin, Panella Vincenzo, Ippolito Giuseppe, Capobianchi Maria Rosaria
Dipartimento di Epidemiologia Ricerca Pre-Clinica e Diagnostica Avanzata, National Institute for Infectious diseases Lazzaro Spallanzani, Rome, Italy.
Department of Infectious Diseases, Istituto Superiore di Sanità, Rome, Italy.
PLoS One. 2017 Nov 10;12(11):e0185428. doi: 10.1371/journal.pone.0185428. eCollection 2017.
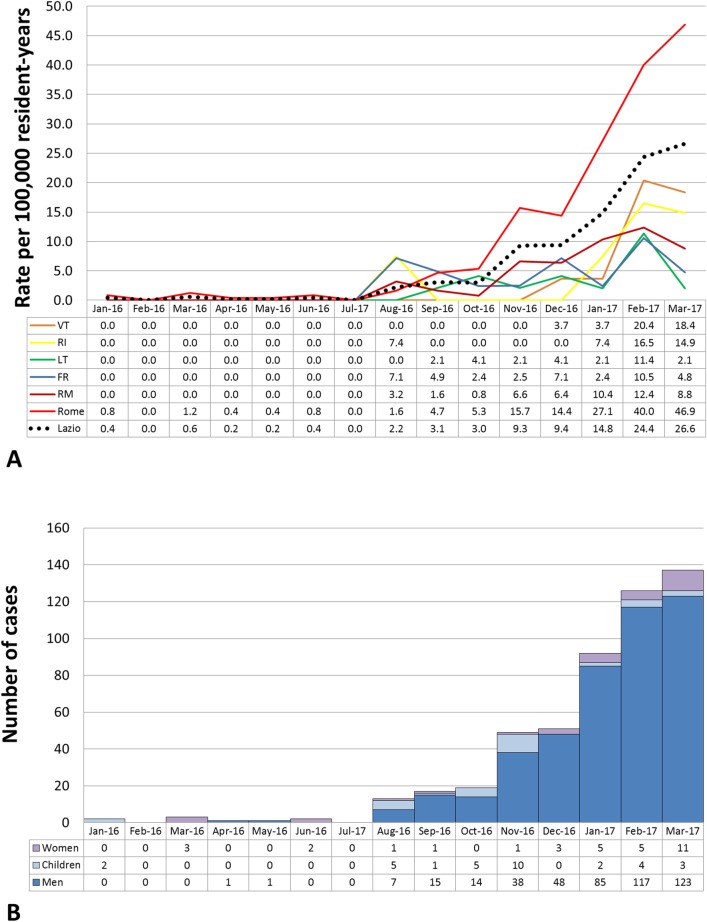
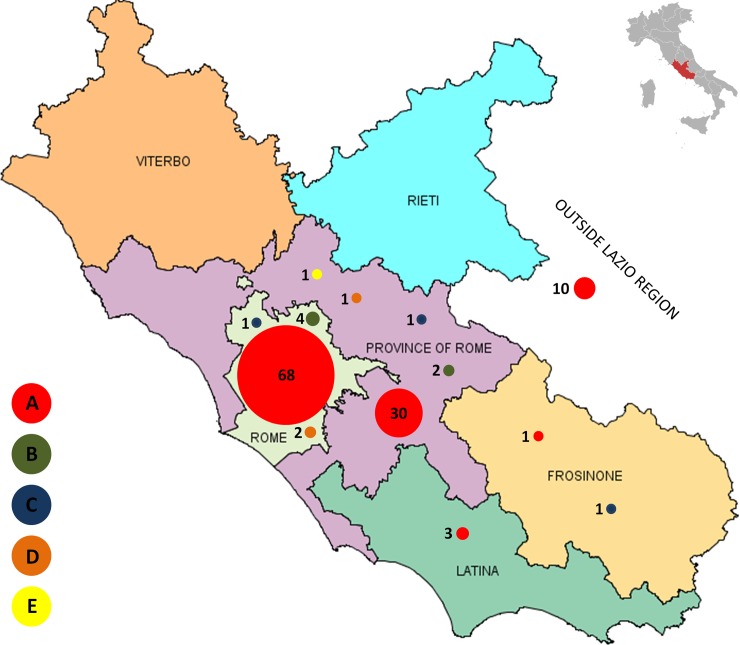
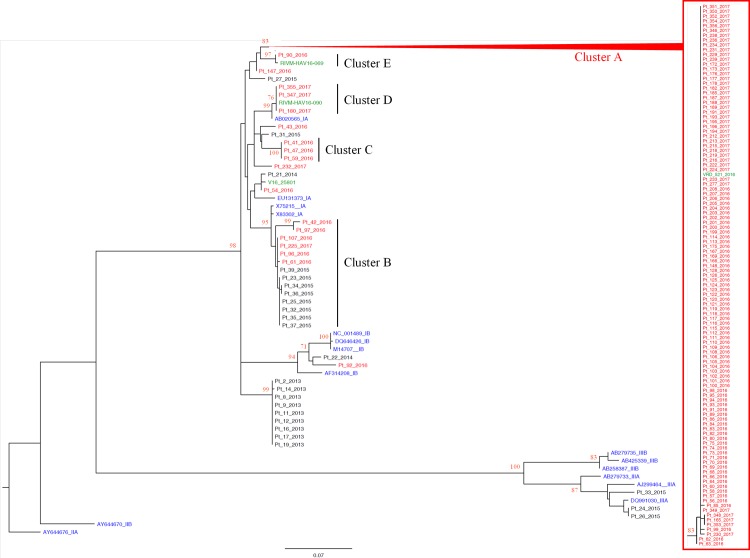
The hepatitis A virus (HAV) is mainly transmitted through the faecal-oral route. In industrialized countries HAV infection generally occurs as either sporadic cases in travelers from endemic areas, local outbreak within closed/semi-closed population and as foodborne community outbreak. Recently, an increasing number of HAV infection clusters have been reported among young men-who-have-sex-with-men (MSM). The Lazio Regional Service for the epidemiology and control for infectious diseases (SeRESMI) has noticed an increase of acute hepatitis A (AHA) since September 2016. Temporal analysis carried out with a discrete Poisson model using surveillance data between January 2016 and March 2017 evidenced an ongoing outbreak of AHA that started at the end of August. Molecular investigation carried out on 130 out of 513 cases AHA reported until March 2017 suggests that this outbreak is mainly supported by an HAV variant which is currently spreading within MSM communities across Europe (VRD_521_2016). The report confirms that AHA is an emerging issue among MSM. In addition through the integration of standard (case based) surveillance with molecular investigation we could discriminate, temporally concomitant but epidemiologically unrelated, clusters due to different HAV variants. As suggested by the WHO, in countries with low HAV circulation, vaccination programmes should be tailored on the local epidemiological patterns to prevent outbreaks among high risk groups and eventual spillover of the infection in the general population.
甲型肝炎病毒(HAV)主要通过粪口途径传播。在工业化国家,甲型肝炎病毒感染通常表现为来自流行地区旅行者的散发病例、封闭/半封闭人群中的局部暴发以及食源性社区暴发。最近,有越来越多的甲型肝炎病毒感染聚集性病例报告发生在男男性行为者(MSM)中。拉齐奥地区传染病流行病学与控制服务局(SeRESMI)注意到自2016年9月以来急性甲型肝炎(AHA)病例有所增加。使用2016年1月至2017年3月的监测数据,通过离散泊松模型进行的时间分析表明,始于8月底的AHA疫情仍在持续。对截至2017年3月报告的513例AHA病例中的130例进行的分子调查表明,此次疫情主要由一种目前正在欧洲MSM社区中传播的甲型肝炎病毒变异株(VRD_521_2016)引起。该报告证实,AHA在MSM中是一个新出现的问题。此外,通过将标准(基于病例)监测与分子调查相结合,我们可以区分由于不同甲型肝炎病毒变异株导致的、在时间上同时发生但在流行病学上无关联的聚集性病例。正如世界卫生组织所建议的,在甲型肝炎病毒传播率较低的国家,应根据当地流行病学模式制定疫苗接种计划,以预防高危人群中的疫情暴发以及感染最终向普通人群的传播。