Tuti Timothy, Agweyu Ambrose, Mwaniki Paul, Peek Niels, English Mike
KEMRI - Wellcome Trust Research Programme, Nairobi, Kenya.
Centre for Health Informatics, Division of Informatics, Imaging & Data Sciences, Faculty of Biology, Medicine and Health, The University of Manchester, Manchester Academic Health Science Centre, Manchester, UK.
BMC Med. 2017 Nov 13;15(1):201. doi: 10.1186/s12916-017-0963-9.
Childhood pneumonia is the leading infectious cause of mortality in children younger than 5 years old. Recent updates to World Health Organization pneumonia guidelines recommend outpatient care for a population of children previously classified as high risk. This revision has been challenged by policymakers in Africa, where mortality related to pneumonia is higher than in other regions and often complicated by comorbidities. This study aimed to identify factors that best discriminate inpatient mortality risk in non-severe pneumonia and explore whether these factors offer any added benefit over the current criteria used to identify children with pneumonia requiring inpatient care.
We undertook a retrospective cohort study of children aged 2-59 months admitted with a clinical diagnosis of pneumonia at 14 public hospitals in Kenya between February 2014 and February 2016. Using machine learning techniques, we analysed whether clinical characteristics and common comorbidities increased the risk of inpatient mortality for non-severe pneumonia. The topmost risk factors were subjected to decision curve analysis to explore if using them as admission criteria had any net benefit above the current criteria.
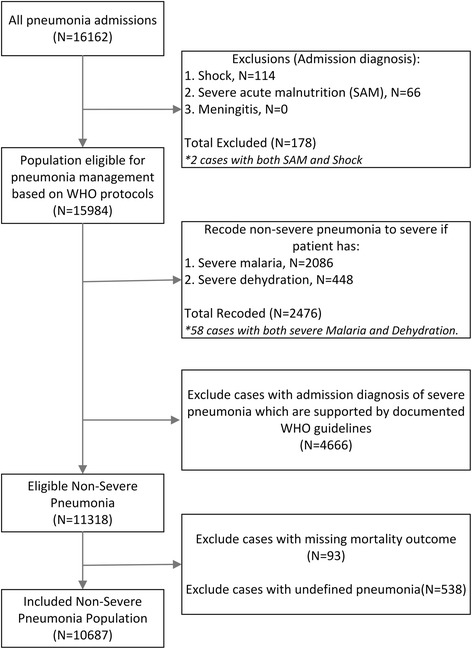
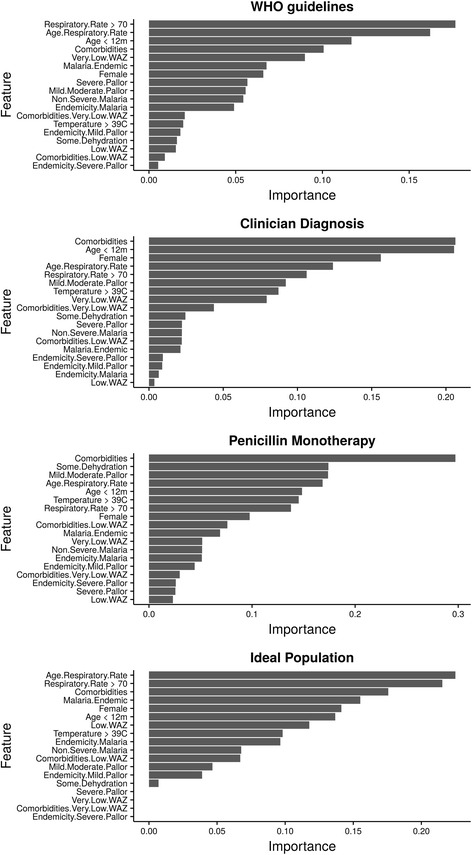
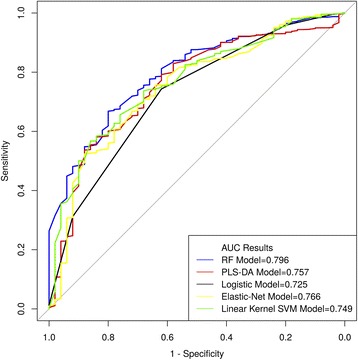
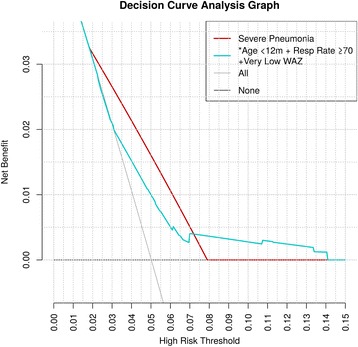
Out of 16,162 children admitted with pneumonia during the study period, 10,687 were eligible for subsequent analysis. Inpatient mortality within this non-severe group was 252/10,687 (2.36%). Models demonstrated moderately good performance; the partial least squares discriminant analysis model had higher sensitivity for predicting mortality in comparison to logistic regression. Elevated respiratory rate (≥70 bpm), age 2-11 months and weight-for-age Z-score (WAZ) < -3SD were highly discriminative of mortality. These factors ranked consistently across the different models. For a risk threshold probability of 7-14%, there is a net benefit to admitting the patient sub-populations with these features as additional criteria alongside those currently used to classify severe pneumonia. Of the population studied, 70.54% met at least one of these criteria. Sensitivity analyses indicated that the overall results were not significantly affected by variations in pneumonia severity classification criteria.
Children with non-severe pneumonia aged 2-11 months or with respiratory rate ≥ 70 bpm or very low WAZ experience risks of inpatient mortality comparable to severe pneumonia. Inpatient care is warranted in these high-risk groups of children.
儿童肺炎是5岁以下儿童死亡的主要感染性病因。世界卫生组织肺炎指南的最新更新建议对以前被归类为高危人群的儿童进行门诊治疗。这一修订受到了非洲政策制定者的质疑,在非洲,与肺炎相关的死亡率高于其他地区,且常伴有合并症。本研究旨在确定能最佳区分非重症肺炎住院死亡风险的因素,并探讨这些因素相对于目前用于确定需要住院治疗的肺炎儿童的标准是否具有任何额外益处。
我们对2014年2月至2016年2月期间在肯尼亚14家公立医院因临床诊断为肺炎而入院的2至59个月大儿童进行了一项回顾性队列研究。使用机器学习技术,我们分析了临床特征和常见合并症是否会增加非重症肺炎住院死亡的风险。对最主要的危险因素进行决策曲线分析,以探讨将它们用作入院标准相对于目前标准是否有任何净益处。
在研究期间因肺炎入院的16162名儿童中,10687名符合后续分析条件。该非重症组的住院死亡率为252/10687(2.36%)。模型表现出中等良好的性能;与逻辑回归相比,偏最小二乘判别分析模型在预测死亡率方面具有更高的敏感性。呼吸频率升高(≥70次/分钟)、年龄2至11个月以及年龄别体重Z评分(WAZ)<-3标准差对死亡率具有高度判别性。这些因素在不同模型中的排名一致。对于7%至14%的风险阈值概率,将具有这些特征的患者亚群作为额外标准与目前用于分类重症肺炎的标准一起纳入收治有净益处。在研究人群中,70.54%至少符合这些标准中的一项。敏感性分析表明,肺炎严重程度分类标准的变化对总体结果没有显著影响。
年龄2至11个月、呼吸频率≥70次/分钟或年龄别体重极低的非重症肺炎儿童经历的住院死亡风险与重症肺炎相当。这些高危儿童群体有必要接受住院治疗。