Botteri Edoardo, Støer Nathalie C, Sakshaug Solveig, Graff-Iversen Sidsel, Vangen Siri, Hofvind Solveig, de Lange Thomas, Bagnardi Vincenzo, Ursin Giske, Weiderpass Elisabete
Norwegian National Advisory Unit for Women's Health, Women's Clinic, Oslo University Hospital, Oslo, Norway.
Department of Bowel Cancer Screening, Cancer Registry of Norway, Oslo University Hospital, Oslo, Norway.
BMJ Open. 2017 Nov 15;7(11):e017639. doi: 10.1136/bmjopen-2017-017639.
With the present study, we aimed to investigate the association between menopausal hormone therapy (HT) and risk of colorectal cancer (CRC).
Cohort study based on the linkage of Norwegian population-based registries.
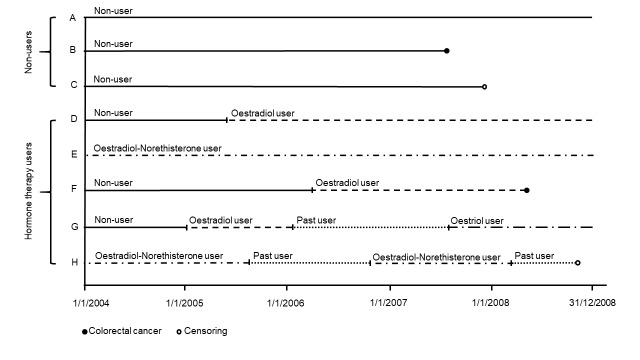
We selected 466822 Norwegian women, aged 55-79, alive and residing in Norway as of 1 January 2004, and we followed them from 2004 to 2008. Each woman contributed person-years at risk as non-user, current user and/or past HT user.
The outcome of interest was adenocarcinoma of the colorectal tract, overall, by anatomic site and stage at diagnosis. Incidence rate ratios (RRs) with 95% CIs were estimated by Poisson regression and were used to evaluate the association between HT and CRC incidence.
During the median follow-up of 4.8 years, 138 655 (30%) women received HT and 3799 (0.8%) incident CRCs occurred. Current, but not past, use of HT was associated with a lower risk of CRC (RR 0.88; 95% CI 0.80 to 0.98). RRs for localised, regionally advanced and metastatic CRC were 1.13 (95% CI 0.91 to 1.41), 0.81 (95% CI 0.70 to 0.94) and 0.79 (95% CI 0.62 to 1.00), respectively. RRs for current use of oestrogen therapy (ET) were 0.91 (95% CI 0.80 to 1.04) while RR for current use of combined oestrogen-progestin therapy (EPT) was 0.85 (95% CI 0.70 to 1.03), as compared with no use of HT. The same figures for ET and EPT in oral formulations were 0.83 (95% CI 0.68 to 1.03) and 0.86 (95% CI 0.71 to 1.05), respectively.
In our nationwide cohort study, HT use lowered the risk of CRC, specifically the most advanced CRC.
通过本研究,我们旨在调查绝经激素治疗(HT)与结直肠癌(CRC)风险之间的关联。
基于挪威人群登记系统关联的队列研究。
我们选取了466822名年龄在55 - 79岁之间、截至2004年1月1日在世且居住在挪威的挪威女性,并在2004年至2008年期间对她们进行随访。每位女性作为非使用者、当前使用者和/或过去的HT使用者贡献了风险人年数。
感兴趣的结局是结直肠腺癌,总体上按诊断时的解剖部位和分期进行统计。通过泊松回归估计发病率比值(RRs)及其95%置信区间(CIs),并用于评估HT与CRC发病率之间的关联。
在中位随访4.8年期间,138655名(30%)女性接受了HT,发生了3799例(0.8%)新发CRC病例。当前(而非过去)使用HT与较低的CRC风险相关(RR 0.88;95% CI 0.80至0.98)。局限性、局部进展期和转移性CRC的RRs分别为1.13(95% CI 0.91至1.41)、0.81(95% CI 0.70至0.94)和0.79(95% CI 0.62至1.00)。与未使用HT相比,当前使用雌激素治疗(ET)的RR为0.91(95% CI 0.80至1.04),而当前使用雌激素 - 孕激素联合治疗(EPT)的RR为0.85(95% CI 0.70至1.03)。口服制剂中ET和EPT的相应数字分别为0.83(95% CI 0.68至1.03)和0.86(95% CI 0.71至1.05)。
在我们的全国性队列研究中,使用HT降低了CRC风险,特别是最晚期CRC的风险。