Department of Obstetrics & Gynecology, McMaster University, 1280 Main St W, HSC 3N52B, Hamilton, ON, L8S 4K1, Canada.
Department of Health Research Methods, Evidence, and Impact, McMaster University, 1280 Main St W, Hamilton, ON, L8S 4K1, Canada.
BMC Pregnancy Childbirth. 2017 Nov 29;17(1):397. doi: 10.1186/s12884-017-1554-7.
Given the controversy around mode of delivery, our objective was to assess the evidence regarding the safest mode of delivery for actively resuscitated extremely preterm cephalic/non-cephalic twin pairs before 28 weeks of gestation.
We searched Cochrane CENTRAL, MEDLINE, EMBASE and http://clinicaltrials.gov from January 1994 to January 2017. Two reviewers independently screened titles, abstracts and full text articles, extracted data and assessed risk of bias. We included randomized controlled trials and observational studies. Our primary outcome was a composite of neonatal death (<28 days of life) and severe brain injury in survivors (intraventricular hemorrhage grade ≥ 3 or periventricular leukomalacia). We performed random-effects meta-analyses, generating odds ratios with 95% confidence intervals for the first and second twin separately, and for both twins together. We assessed the risk of bias using a modified Newcastle Ottawa Scale (NOS) for observational studies and used Grading of Recommendations Assessment, Development and Evaluation approach (GRADE).
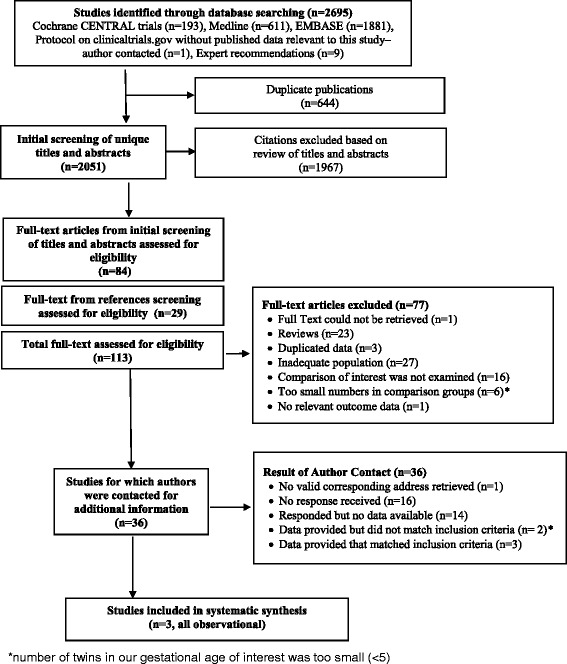
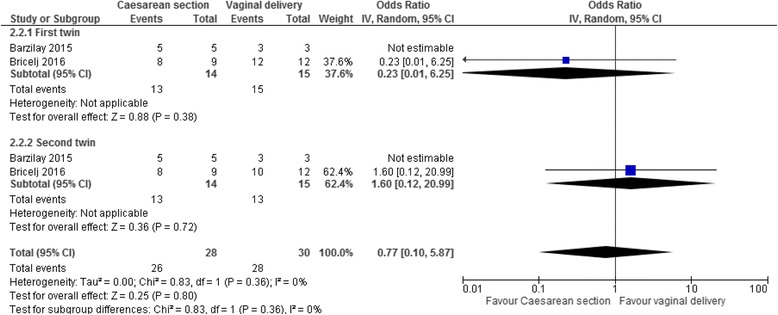
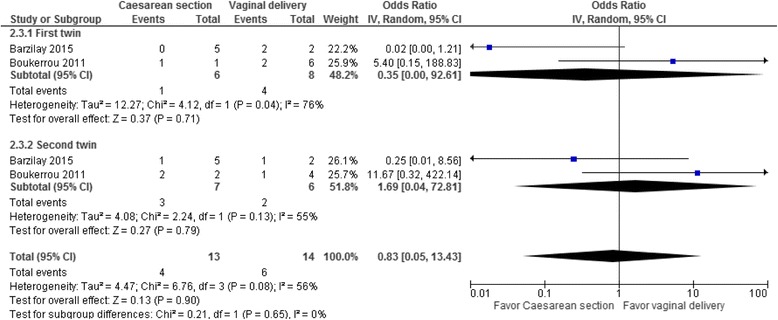
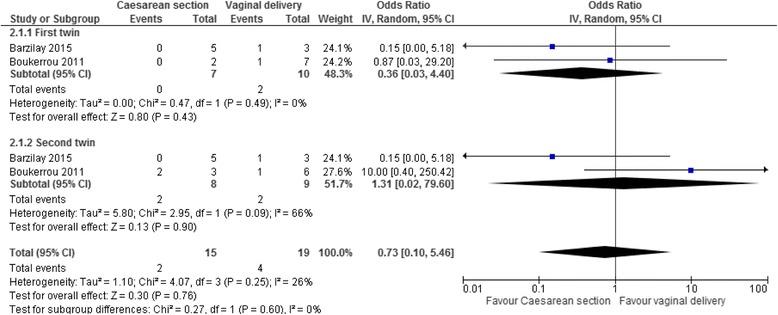
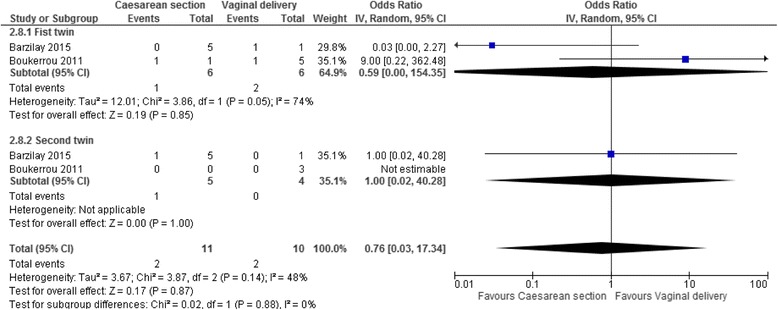
Our search generated 2695 articles, and after duplicate removal, we screened 2051 titles and abstracts, selecting 113 articles for full-text review. We contacted 36 authors, and ultimately, three observational studies met our inclusion criteria. In cephalic/non-cephalic twin pairs delivered by caesarean section compared to vaginal birth at 24-27 weeks the odds ratio for our composite outcome of neonatal death and severe brain injury for the cephalic first twin was 0.35 (95% CI 0.00-92.61, two studies, I = 76%), 1.69 for the non-cephalic second twin (95% CI 0.04-72.81, two studies, I = 55%) and 0.83 for both twins (95% CI 0.05-13.43, two studies, I = 56%). According to the modified Newcastle Ottawa Scale we assessed individual study quality as being at high risk of bias and according to GRADE the overall evidence for our primary outcomes was very low.
Our systematic review on the safest mode of delivery for extremely preterm cephalic/non-cephalic twin pairs found very limited existing evidence, without significant differences in neonatal death and severe brain injury by mode of delivery.
鉴于分娩方式存在争议,我们的目的是评估在 28 周前积极复苏的极早产儿头位/非头位双胎的最安全分娩方式的证据。
我们检索了 Cochrane 中心、MEDLINE、EMBASE 和 http://clinicaltrials.gov,检索时间从 1994 年 1 月到 2017 年 1 月。两位审查员独立筛选标题、摘要和全文文章,提取数据并评估偏倚风险。我们纳入了随机对照试验和观察性研究。我们的主要结局是新生儿死亡(<28 天)和幸存者严重脑损伤(脑室出血 3 级或脑室内白质软化)的复合结局。我们对每个双胞胎和双胞胎整体分别进行了随机效应荟萃分析,生成了优势比及其 95%置信区间。我们使用改良的纽卡斯尔-渥太华量表(NOS)评估观察性研究的偏倚风险,并使用推荐评估、制定与评估分级(GRADE)方法评估证据质量。
我们的检索生成了 2695 篇文章,经过重复去除后,我们筛选了 2051 篇标题和摘要,选择了 113 篇全文进行审查。我们联系了 36 位作者,最终有 3 项观察性研究符合纳入标准。在 24-27 周行剖宫产分娩的头位/非头位双胎中,头位第一胎的新生儿死亡和严重脑损伤复合结局的优势比为 0.35(95%CI 0.00-92.61,两项研究,I=76%),非头位第二胎为 1.69(95%CI 0.04-72.81,两项研究,I=55%),双胞胎整体为 0.83(95%CI 0.05-13.43,两项研究,I=56%)。根据改良的纽卡斯尔-渥太华量表,我们评估单个研究质量为高偏倚风险,根据 GRADE,我们主要结局的总体证据质量非常低。
我们对极早产儿头位/非头位双胎最安全分娩方式的系统评价发现,现有证据非常有限,分娩方式对新生儿死亡和严重脑损伤无显著差异。