Burger Charles D, Ghandour Mohamedanwar, Padmanabhan Menon Divya, Helmi Haytham, Benza Raymond L
Division of Pulmonary, Allergy and Sleep Medicine, Mayo Clinic.
Department of Internal Medicine, Mayo Clinic.
Clinicoecon Outcomes Res. 2017 Nov 24;9:731-739. doi: 10.2147/CEOR.S119117. eCollection 2017.
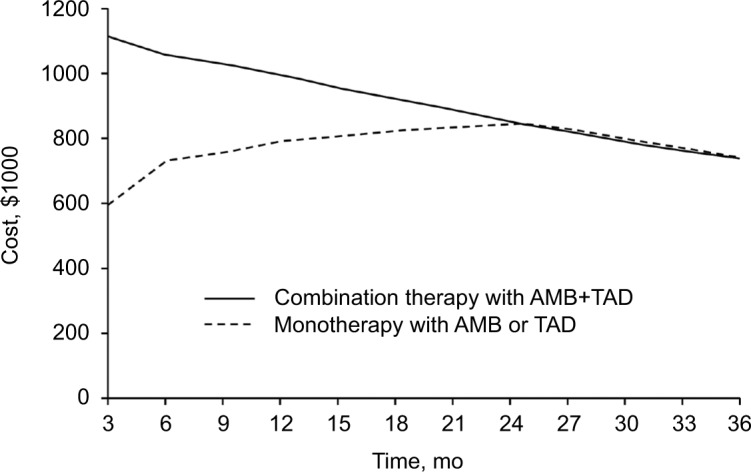
Pulmonary arterial hypertension (PAH) has a high morbidity rate and is fatal if left untreated. Increasing evidence supports early intervention, possibly with initial combination therapy. PAH-specific pharmaceuticals, however, are expensive and may have serious adverse effects, particularly when used in combination. The currently dynamic health care economy reinforces the need for a review of early intervention from both outcomes and economic perspectives. We aimed to review the clinical and economic impact of PAH therapy, particularly examining drug cost, hospitalization burden, and health care economics impact, and the effect of early intervention on clinical outcomes. We searched PubMed, Scopus, Ovid, and MEDLINE databases from 2005 to 2017 for studies comparing drug cost, clinical outcomes, and hospitalization burden associated with therapy for PAH. Emerging data indicate that early therapy is effective, but drug therapy is expensive, particularly with combination therapy. Efficacy studies also generally show benefit of combination therapy for patients in World Health Organization functional class II, with a consistent decrease in hospitalization. Pharmacoeconomic studies are limited but indicate that increased pharmacy costs are at least partially offset by decreased health care utilization, particularly inpatient care. Modeling also shows a cost benefit with combination therapy at 2 years. Nonetheless, more rigorously collected health care economic data should be incorporated into future drug efficacy trials to provide a clearer understanding of the impact and the associated cost benefit of early PAH therapy. Increasing evidence in support of early intervention and combination therapy for PAH is associated with rising medication costs that are largely offset by reduced hospitalization, on the basis of the currently available literature. Nonetheless, the studies performed to date have methodologic limitations that highlight the need for prospective studies using more robust economic modeling.
肺动脉高压(PAH)发病率高,若不治疗会导致死亡。越来越多的证据支持早期干预,可能采用初始联合治疗。然而,PAH特异性药物价格昂贵,且可能有严重不良反应,尤其是联合使用时。当前动态的医疗保健经济状况强化了从结果和经济角度对早期干预进行审查的必要性。我们旨在回顾PAH治疗的临床和经济影响,尤其考察药物成本、住院负担和医疗保健经济学影响,以及早期干预对临床结果的影响。我们检索了2005年至2017年的PubMed、Scopus、Ovid和MEDLINE数据库,以查找比较PAH治疗相关药物成本、临床结果和住院负担的研究。新出现的数据表明早期治疗是有效的,但药物治疗成本高昂,尤其是联合治疗。疗效研究通常也显示联合治疗对世界卫生组织功能分级为II级的患者有益,住院次数持续减少。药物经济学研究有限,但表明药房成本的增加至少部分被医疗保健利用率的降低所抵消,尤其是住院治疗。模型还显示联合治疗在2年时有成本效益。尽管如此,更严格收集的医疗保健经济数据应纳入未来的药物疗效试验,以更清楚地了解早期PAH治疗的影响及其相关成本效益。根据现有文献,越来越多支持PAH早期干预和联合治疗的证据与药物成本上升相关,而住院次数减少在很大程度上抵消了这一成本。尽管如此,迄今为止进行的研究存在方法学局限性,这突出了使用更稳健的经济模型进行前瞻性研究的必要性。