Department of Pathology, University of Otago, Christchurch, PO Box 4345, Christchurch, 8140, New Zealand.
Department of Intensive Care Medicine, Christchurch Hospital, Private Bag 4710, Christchurch, 8140, New Zealand.
Crit Care. 2017 Dec 11;21(1):300. doi: 10.1186/s13054-017-1891-y.
Vitamin C is an essential water-soluble nutrient which cannot be synthesised or stored by humans. It is a potent antioxidant with anti-inflammatory and immune-supportive roles. Previous research has indicated that vitamin C levels are depleted in critically ill patients. In this study we have assessed plasma vitamin C concentrations in critically ill patients relative to infection status (septic shock or non-septic) and level of inflammation (C-reactive protein concentrations). Vitamin C status was also assessed relative to daily enteral and parenteral intakes to determine if standard intensive care unit (ICU) nutritional support is adequate to meet the vitamin C needs of critically ill patients.
Forty-four critically ill patients (24 with septic shock, 17 non-septic, 3 uncategorised) were recruited from the Christchurch Hospital Intensive Care Unit. We measured concentrations of plasma vitamin C and a pro-inflammatory biomarker (C-reactive protein) daily over 4 days and calculated patients' daily vitamin C intake from the enteral or total parenteral nutrition they received. We compared plasma vitamin C and C-reactive protein concentrations between septic shock and non-septic patients over 4 days using a mixed effects statistical model, and we compared the vitamin C status of the critically ill patients with known vitamin C bioavailability data using a four-parameter log-logistic response model.
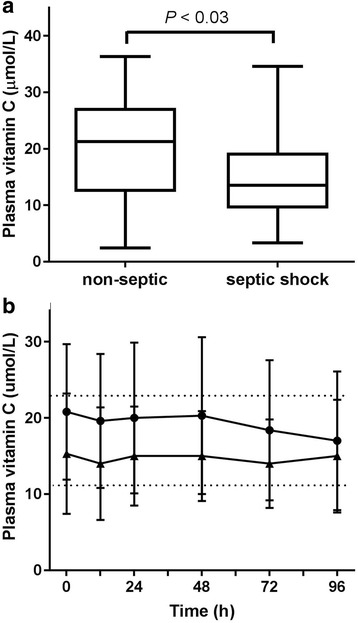
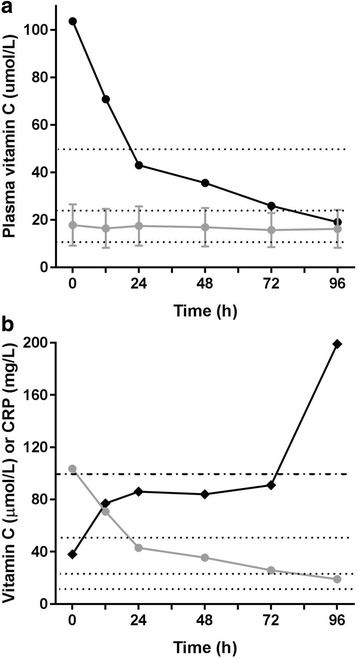
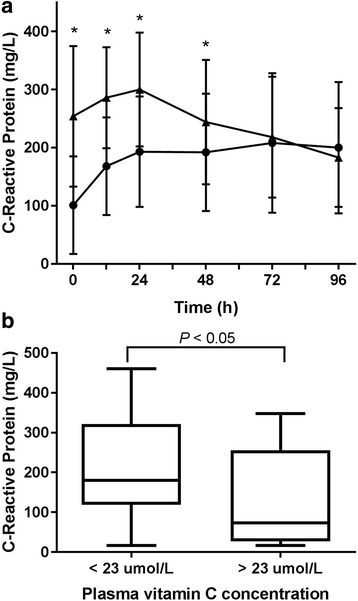
Overall, the critically ill patients exhibited hypovitaminosis C (i.e., < 23 μmol/L), with a mean plasma vitamin C concentration of 17.8 ± 8.7 μmol/L; of these, one-third had vitamin C deficiency (i.e., < 11 μmol/L). Patients with hypovitaminosis C had elevated inflammation (C-reactive protein levels; P < 0.05). The patients with septic shock had lower vitamin C concentrations and higher C-reactive protein concentrations than the non-septic patients (P < 0.05). Nearly 40% of the septic shock patients were deficient in vitamin C, compared with 25% of the non-septic patients. These low vitamin C levels were apparent despite receiving recommended intakes via enteral and/or parenteral nutritional therapy (mean 125 mg/d).
Critically ill patients have low vitamin C concentrations despite receiving standard ICU nutrition. Septic shock patients have significantly depleted vitamin C levels compared with non-septic patients, likely resulting from increased metabolism due to the enhanced inflammatory response observed in septic shock.
维生素 C 是一种必需的水溶性营养素,人体无法合成或储存。它是一种有效的抗氧化剂,具有抗炎和免疫支持作用。先前的研究表明,危重症患者的维生素 C 水平会耗尽。在这项研究中,我们评估了危重症患者的血浆维生素 C 浓度与感染状态(感染性休克或非感染性)和炎症水平(C 反应蛋白浓度)的关系。还评估了维生素 C 状态与每日肠内和肠外摄入的关系,以确定标准重症监护病房(ICU)营养支持是否足以满足危重症患者的维生素 C 需求。
从克赖斯特彻奇医院重症监护病房招募了 44 名危重症患者(24 名感染性休克,17 名非感染性,3 名未分类)。我们在 4 天内每天测量血浆维生素 C 和促炎生物标志物(C 反应蛋白)的浓度,并根据他们接受的肠内或全胃肠外营养计算患者的每日维生素 C 摄入量。我们使用混合效应统计模型比较了 4 天内感染性休克和非感染性患者的血浆维生素 C 和 C 反应蛋白浓度,并使用四参数对数逻辑响应模型将危重症患者的维生素 C 状态与已知的维生素 C 生物利用度数据进行了比较。
总体而言,危重症患者表现出维生素 C 不足(即<23 μmol/L),平均血浆维生素 C 浓度为 17.8±8.7 μmol/L;其中三分之一患者存在维生素 C 缺乏症(即<11 μmol/L)。维生素 C 不足的患者炎症水平升高(C 反应蛋白水平;P<0.05)。感染性休克患者的维生素 C 浓度较低,C 反应蛋白浓度较高,而非感染性患者(P<0.05)。近 40%的感染性休克患者存在维生素 C 缺乏症,而非感染性患者为 25%。尽管通过肠内和/或肠外营养治疗给予了推荐的摄入量(平均 125mg/d),但仍存在这些低维生素 C 水平。
尽管接受了标准 ICU 营养支持,危重症患者的维生素 C 浓度仍较低。感染性休克患者的维生素 C 水平明显低于非感染性休克患者,这可能是由于感染性休克中观察到的炎症反应增强导致代谢增加所致。