Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, 1275 York Avenue, New York, NY, 10065, USA.
Immunology, Memorial Sloan Kettering Cancer Center, New York, USA.
J Immunother Cancer. 2018 Jan 3;6(1):1. doi: 10.1186/s40425-017-0311-9.
Cytokine release syndrome (CRS) has been reported after immunologic manipulations, most often through therapeutic monoclonal antibodies. To our knowledge, CRS after radiation therapy (RT) for cancer has not been reported before. The development of unusual clinical signs and symptoms after RT led us to investigate the possibility of CRS after RT and review the medical literature on this topic.
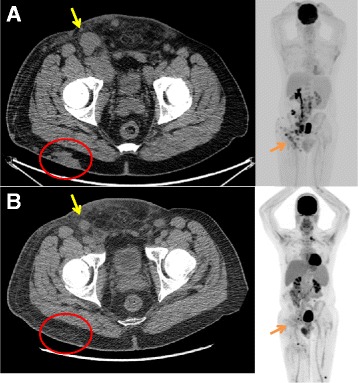
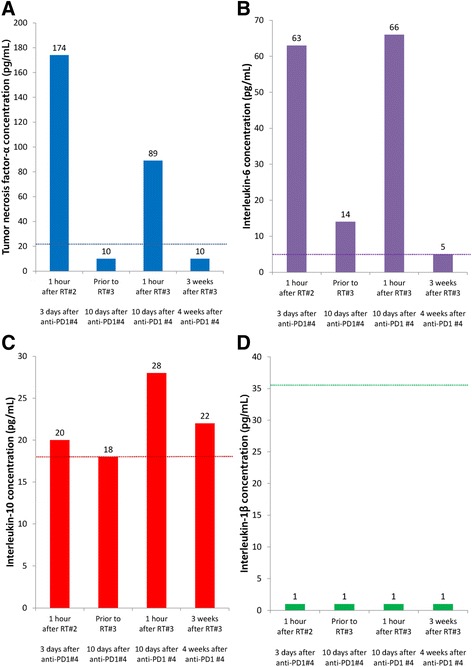
A 65 year-old man with untreated chronic lymphocytic leukemia and recurrent, metastatic Merkel cell carcinoma undergoing anti-programmed death 1 (PD1) immunotherapy was referred for palliative RT to sites of progressing metastases. Within hours of each weekly dose of RT, he experienced fever, tachycardia, hypotension, rash, dyspnea, and rigors. Based on clinical suspicion for CRS, blood cytokine measurements were performed 1 h after the second and third dose of RT and demonstrated tumor necrosis factor alpha (TNF-α) and interleukin-6 (IL-6) levels approximately ten-fold higher than normal. These were near normal immediately prior to the third dose of RT, and resolved to normal levels 3 weeks after RT. He experienced rapid regression of irradiated tumors, with development of new sites of metastases soon thereafter. A literature review revealed no clinical cases of CRS after RT for cancer.
RT during anti-PD1 immunotherapy in a patient with underlying immune dysfunction appeared to be the putative mediator of an immune process which yielded significant increases in pro-inflammatory cytokines, and produced the clinical symptoms meeting the definition of grade 3 CRS. This case demonstrates the capability of RT to elicit immune-related adverse events.
细胞因子释放综合征 (CRS) 已在免疫治疗后被报道,最常见的是通过治疗性单克隆抗体。据我们所知,癌症放射治疗 (RT) 后尚未有 CRS 的报道。在 RT 后出现不寻常的临床症状和体征,促使我们研究 RT 后发生 CRS 的可能性,并对该主题的医学文献进行回顾。
一名 65 岁男性,患有未经治疗的慢性淋巴细胞白血病和复发性转移性 Merkel 细胞癌,正在接受抗程序性死亡 1 (PD1) 免疫治疗,因进展性转移灶而行姑息性 RT。在每周接受 RT 治疗后的数小时内,他出现发热、心动过速、低血压、皮疹、呼吸困难和寒战。根据对 CRS 的临床怀疑,在接受 RT 治疗的第二和第三次剂量后 1 小时进行了血液细胞因子测量,结果显示肿瘤坏死因子-α (TNF-α) 和白细胞介素-6 (IL-6) 水平比正常值高约十倍。在第三次 RT 剂量前接近正常,并在 RT 后 3 周内恢复到正常水平。他经历了照射肿瘤的快速消退,随后很快出现新的转移部位。文献复习未发现癌症 RT 后发生 CRS 的临床病例。
在有潜在免疫功能障碍的患者中,在接受抗 PD1 免疫治疗的同时进行 RT,似乎是一种免疫过程的潜在介导因素,该过程导致促炎细胞因子显著增加,并产生符合 3 级 CRS 定义的临床症状。该病例表明 RT 具有引发免疫相关不良事件的能力。