Pajulammi Hanna M, Pihlajamäki Harri K, Luukkaala Tiina H, Jousmäki Janne J, Jokipii Pekka H, Nuotio Maria S
Department of Geriatric Medicine, Seinäjoki Central Hospital, Seinäjoki, Finland.
Division of Orthopedics and Traumatology, Seinäjoki Central Hospital, Seinäjoki, Finland.
Geriatr Orthop Surg Rehabil. 2017 Dec;8(4):183-191. doi: 10.1177/2151458517716516. Epub 2017 Sep 7.
To examine the association of patient-related factors with the effect of an in-hospital comprehensive geriatric assessment (CGA) on hip fracture mortality.
Population-based, prospective data were collected on 1425 consecutive hip fracture patients aged ≥65 in a central hospital providing orthogeriatric service. Outcome was mortality at 1 month after hip fracture associated with receiving versus not receiving CGA.
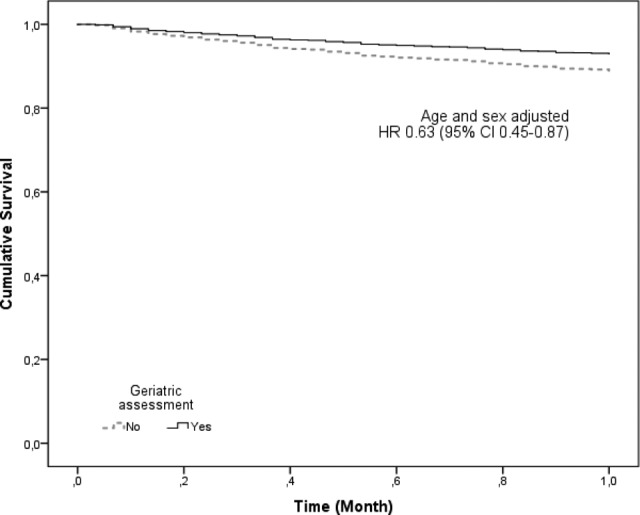
Of the patients receiving CGA compared to those who did not, 8.5% versus12.0% had died within 1 month of the hip fracture ( = .028). In the age- and sex-adjusted Cox proportional hazards model, CGA was associated with a decreased risk of 1-month mortality in patients aged 80 to 89 years (hazard ratio [HR] 0.46, 95% confidence interval [CI]: 0.29-0.73), females (HR: 0.57, 95% CI: 0.38-0.86), having American Society of Anesthesiologists (ASA) score 1 to 3 (HR: 0.60, 95% CI: 0.37-0.99), taking 4 to 10 daily medications (HR: 0.59, 95% CI: 0.38-0.91), with a diagnosis of memory disorder (HR: 0.50, 95% CI: 0.29-0.88), with an estimated glomerular filtration rate <30 mL/min/1.73m (HR: 0.28, 95% CI: 0.10-0.76), or living in an assisted living accommodation (HR: 0.40, 95% CI: 0.21-0.76).
Several modifiable and patient-related factors were associated with decreased risk of 1-month mortality when CGA was performed during hospitalization for hip fracture. Between "younger and fitter" and "oldest and frailest," there is a large group of hip fracture patients whose survival can be improved by in-hospital CGA.
探讨患者相关因素与住院期间综合老年评估(CGA)对髋部骨折死亡率影响之间的关联。
在一家提供老年骨科服务的中心医院,收集了1425例年龄≥65岁的连续性髋部骨折患者的基于人群的前瞻性数据。结局指标为髋部骨折后1个月内接受与未接受CGA相关的死亡率。
与未接受CGA的患者相比,接受CGA的患者在髋部骨折后1个月内的死亡率分别为8.5%和12.0%(P = 0.028)。在年龄和性别调整的Cox比例风险模型中,CGA与80至89岁患者1个月死亡率风险降低相关(风险比[HR] 0.46,95%置信区间[CI]:0.29 - 0.73)、女性(HR:0.57,95% CI:0.38 - 0.86)、美国麻醉医师协会(ASA)评分为1至3分(HR:0.60,95% CI:0.37 - 0.99)、每日服用4至10种药物(HR:0.59,95% CI:0.38 - 0.91)、诊断为记忆障碍(HR:0.50,95% CI:0.29 - 0.88)、估计肾小球滤过率<30 mL/min/1.73m²(HR:0.28,95% CI:0.10 - 0.76)或居住在辅助生活机构(HR:0.40,95% CI:0.21 - 0.76)相关。
在髋部骨折住院期间进行CGA时,一些可改变的患者相关因素与1个月死亡率风险降低相关。在“较年轻且健康状况较好”和“最年长且最虚弱”之间,有一大组髋部骨折患者的生存情况可通过住院期间的CGA得到改善。