Weiji Qiu, Shitong Li, Yu Luo, Tianfang Hua, Ning Kong, Lina Zhang
Department of Anesthesia and Critical Care Medicine, Shanghai Fourth People's Hospital, 1878 North Sichuan Road, Hongkou District, Shanghai, 200081, China.
Department of Anesthesia, Shanghai First People's Hospital affiliated to Shanghai Jiaotong University School of Medcine, 100 Haining Road, Hongkou District, Shanghai, 200080, China.
BMC Anesthesiol. 2018 Jan 12;18(1):6. doi: 10.1186/s12871-018-0470-3.
Surgical patients are asked to fast for a sufficient duration to ensure that the amount of residual liquid in the stomach is within the safe range, thereby reducing the risk of gastric reflux perioperatively. The authors hypothesized that subjective hunger numerical rating scale (NRS) score could also help assess the process of gastric emptying and determine the amount of fluid remaining in the stomach.
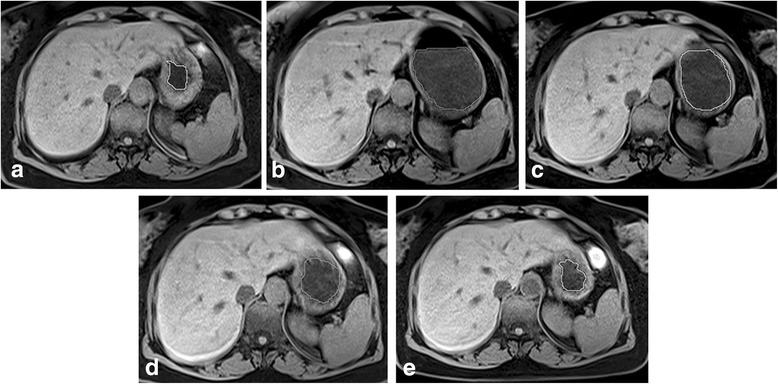
The current study consisted of healthy volunteers recruited by advertisement and mutual introduction. Participants were asked to rate their subjective hunger feeling every 30 min after oral administration of 8 mL/kg carbohydrate nutrient solution that contained 10% maltodextrin and 2.5% sucrose. Consecutively, the gastric residual fluid was measured by magnetic resonance imagining (MRI). The Spearman's correlation coefficient, the ROC curves and the stepwise regression were used to analyze the predictive value of NRS for the gastric emptying process.
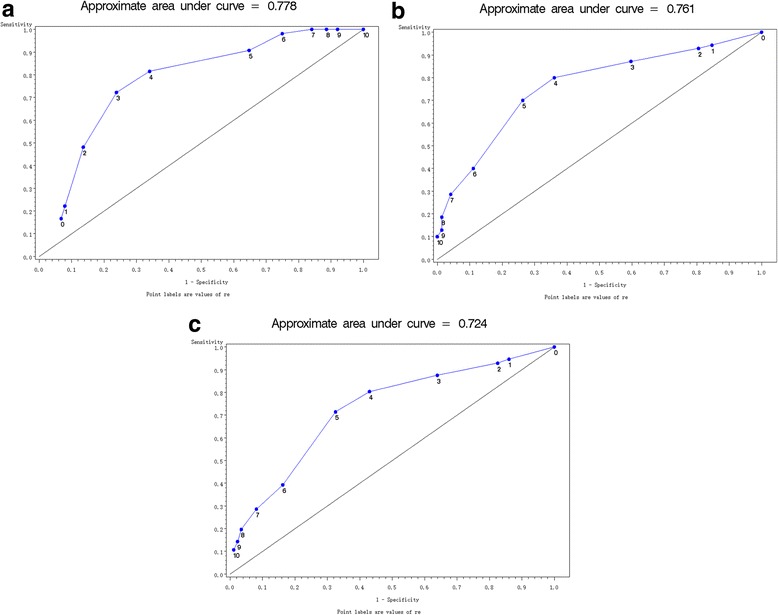
The cohort consisted of 29 healthy volunteers enrolled in this study. The area under ROC curves estimated by the NRS score for the gastric residual volume of 2 mL/kg, 1 mL/kg, and 0.5 mL/kg were AUC = 0.78, AUC = 0.76, and AUC = 0.72, respectively. The correlation coefficient between the NRS score and the residual liquid in the stomach was -0.57 (P < 0.01). The correlation coefficient between the increase of the NRS score and the decrease of gastric liquid residual volume was 0.46 (P < 0.01). The standardized estimate of NRS score for the residual volume was -0.18 (P < 0.01) and the standardized estimate of fasting time was -0.73 (P < 0.01).
The subjective hunger NRS score can not accurately predict the gastric residual volume, but it can provide a reference for clinicians to judge the gastric emptying process and it should be used as a second check after oral intake of clear fluids before surgery according to the new fasting protocol.
要求外科手术患者禁食足够长的时间,以确保胃内残余液体量在安全范围内,从而降低围手术期胃反流的风险。作者推测,主观饥饿数字评定量表(NRS)评分也有助于评估胃排空过程,并确定胃内剩余液体量。
本研究由通过广告招募和相互介绍的健康志愿者组成。参与者在口服含有10%麦芽糊精和2.5%蔗糖的8 mL/kg碳水化合物营养液后,每30分钟对其主观饥饿感进行评分。随后,通过磁共振成像(MRI)测量胃残余液体。采用Spearman相关系数、ROC曲线和逐步回归分析NRS对胃排空过程的预测价值。
本研究纳入了29名健康志愿者。NRS评分对胃残余量2 mL/kg、1 mL/kg和0.5 mL/kg的ROC曲线下面积分别为AUC = 0.78、AUC = 0.76和AUC = 0.72。NRS评分与胃内残余液体的相关系数为-0.57(P < 0.01)。NRS评分增加与胃液体残余量减少的相关系数为0.46(P < 0.01)。残余量的NRS评分标准化估计值为-0.18(P < 0.01),禁食时间的标准化估计值为-0.73(P < 0.01)。
主观饥饿NRS评分不能准确预测胃残余量,但可为临床医生判断胃排空过程提供参考,应根据新的禁食方案在术前口服清亮液体后作为二次检查使用。