Work ability and working careers, Finnish Institute of Occupational Health, PL 40, 00251, Helsinki, Finland.
Creating Solutions, Statistics and Health Economics Team, Finnish Institute of Occupational Health, Helsinki, Finland.
BMC Public Health. 2018 Jan 17;18(1):152. doi: 10.1186/s12889-018-5059-8.
Previous studies have not distinguished between different alcohol-use histories, which could have contributed to the current inconsistent evidence regarding the relationship between alcohol use and subsequent sickness absence. We thus examined alcohol use and subsequent diagnosis-specific sickness absence in groups with different levels of alcohol use, as well as in lifelong abstainers, former drinkers, and people with clinical alcohol use disorders.
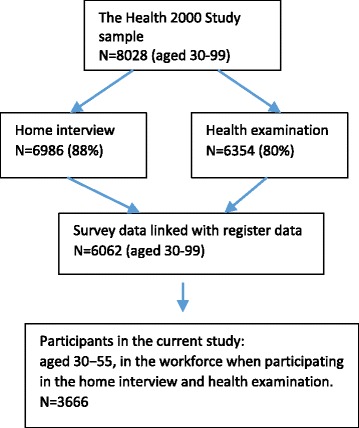
The data of the population-based Health 2000 Survey (BRIF8901) of 3666 Finns aged 30-55 were linked with national registers on medically certified sickness absences lasting for > 10 working days (long-term) for all causes (2000 - 2010) and for mental or musculoskeletal disorders (2004-2010), as well as with registers on pensions and death (2000-2010). Alcohol use was assessed by questionnaire. Chronic somatic diseases were evaluated at baseline in a clinical examination, and common mental and alcohol use disorders using the Composite International Diagnostic Interview (CIDI). Cox regression analyses were conducted with censoring for death and retirement from work.
During an average 10-year follow-up, 56.0% of the participants had at least one long-term sickness absence period. Compared with light drinkers, those having an alcohol use disorder had increased risk of all-cause sickness absence (HR = 1.27; 95% CI = 1.04 - 1.54) and sickness absence due to mental disorders (HR = 2.16; 95% CI = 1.39 - 3.35), when somatic and mental disorders as well as demographic, lifestyle-related and occupational factors at baseline were accounted for. Lifelong abstainers did not differ from light drinkers. Also high-volume drinking (HR = 1.52; 95% CI 1.03 - 2.25) and former drinking (HR = 1.57; 95% CI = 1.15 - 2.15) were associated with long-term sickness absence due to mental disorders. Alcohol use was not predictive of sickness absence due to musculoskeletal disorders.
These results highlight the need to distinguish between former drinking and lifelong abstinence, as only former drinking was associated with sickness absence. Alcohol use disorder and high-volume drinking were strongly predictive of sickness absence due to mental disorders. Identifying people with excessive alcohol use e.g. in occupational health care, and mapping and supporting their mental health may help in preventing sickness absences.
先前的研究并未区分不同的饮酒史,这可能导致目前关于饮酒与随后缺勤之间关系的证据不一致。因此,我们研究了不同饮酒水平组、终身戒酒者、前饮酒者和有临床酒精使用障碍者的饮酒与随后特定疾病缺勤之间的关系。
对 3666 名年龄在 30-55 岁的芬兰人进行了基于人群的健康 2000 调查(BRIF8901)的数据,这些人被链接到全国记录,记录了所有原因(2000-2010 年)和精神或肌肉骨骼疾病(2004-2010 年)持续超过 10 个工作日的经医学证明的长期病假(长期),以及养老金和死亡登记(2000-2010 年)。饮酒情况通过问卷调查进行评估。在基线时,通过临床检查评估慢性躯体疾病,通过复合国际诊断访谈(CIDI)评估常见的精神和酒精使用障碍。对死亡和退休进行 censoring 后,采用 Cox 回归分析。
在平均 10 年的随访期间,56.0%的参与者至少有一次长期病假。与轻度饮酒者相比,有酒精使用障碍者患所有原因病假(HR=1.27;95%CI=1.04-1.54)和精神障碍病假(HR=2.16;95%CI=1.39-3.35)的风险增加,同时还考虑了基线时的躯体和精神障碍以及人口统计学、生活方式相关和职业因素。终身戒酒者与轻度饮酒者无差异。此外,大量饮酒(HR=1.52;95%CI 1.03-2.25)和以前饮酒(HR=1.57;95%CI=1.15-2.15)也与精神障碍导致的长期病假有关。饮酒与肌肉骨骼疾病导致的病假无关。
这些结果强调需要区分以前的饮酒和终身戒酒,因为只有以前的饮酒与病假有关。酒精使用障碍和大量饮酒与精神障碍导致的病假有很强的预测性。例如,在职业保健中识别过度饮酒者,并对其心理健康进行评估和支持,可能有助于预防病假。