Fagoni Nazzareno, Piva Simone, Peli Elena, Turla Fabio, Pecci Elisabetta, Gualdoni Livio, Fiorese Bertilla, Rasulo Frank, Latronico Nicola
Department of Anesthesia, Critical Care and Emergency, Spedali Civili University Hospital, Piazzale Ospedali Civili, 1, 23123, Brescia, Italy.
Department of Molecular and Translational Medicine, University of Brescia, Brescia, Italy.
Ann Intensive Care. 2018 Jan 22;8(1):11. doi: 10.1186/s13613-018-0354-1.
Weaning protocols expedite extubation in mechanically ventilated patients, yet the literature investigating the application in tracheostomized patients remains scarce. The primary objective of this parallel randomized controlled pilot trial (RCT) was to assess the feasibility and safety of a nurse-led weaning protocol (protocol) compared to weaning based on physician's clinical judgment (control) in tracheostomized critically ill patients.
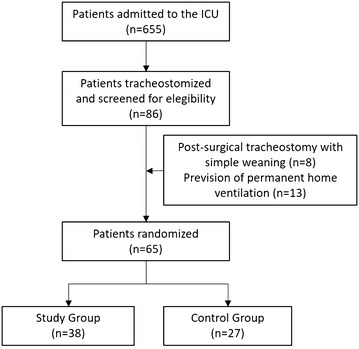
We enrolled 65 patients, 27 were in the protocol group and 38 in the control group. Of 27 patients in the protocol group, 1 (3.7%) died in the ICU, 24 (88.9%) were successfully weaned from tracheostomy, and 2 (7.4%) were transferred still on the ventilator. Of 38 patients in the control group, 2 (5.3%) died in the ICU, 22 (57.9%) were successfully weaned from tracheostomy, and 14 were transferred still on the ventilator (36.8%). Risk of being discharged from the ICU on the ventilator was higher in the control group (relative risk: 1.5, IC 95% 1.14-2.01). Concerning safety and feasibility, no patients were excluded after randomization. There was no crossover between the two study arms nor missing data, and no severe adverse event related to the study protocol application was recorded by the staff. Weaning time and rate of successful weaning were not different in the protocol group compared to the control group (long-rank test, p = 0.31 for MV duration, p = 0.45 for weaning time). Based on our results and assuming a 30% reduction of the weaning time for the protocol group, 280 patients would be needed for a RCT to establish efficacy.
In this pilot RCT we demonstrated that a nurse-led weaning protocol from tracheostomy was feasible and safe. A larger RCT is justified to assess efficacy.
撤机方案可加快机械通气患者的拔管进程,但关于其在气管切开患者中的应用研究仍较为匮乏。这项平行随机对照试验(RCT)的主要目的是评估在气管切开的重症患者中,由护士主导的撤机方案(试验组)相较于基于医生临床判断的撤机方式(对照组)的可行性和安全性。
我们共纳入65例患者,试验组27例,对照组38例。试验组的27例患者中,1例(3.7%)在重症监护病房(ICU)死亡,24例(88.9%)成功脱机,2例(7.4%)仍使用呼吸机转院。对照组的38例患者中,2例(5.3%)在ICU死亡,22例(57.9%)成功脱机,14例(36.8%)仍使用呼吸机转院。对照组患者带机离开ICU的风险更高(相对风险:1.5,95%置信区间1.14 - 2.01)。在安全性和可行性方面,随机分组后无患者被排除。两组之间没有交叉情况,也没有数据缺失,工作人员未记录到与研究方案应用相关的严重不良事件。试验组与对照组的撤机时间和成功撤机率无差异(对数秩检验,机械通气时间p = 0.31,撤机时间p = 0.45)。根据我们的研究结果,并假设试验组撤机时间减少30%,则需要280例患者进行RCT以确定疗效。
在这项RCT试验中,我们证明了由护士主导的气管切开撤机方案是可行且安全的。有必要开展更大规模的RCT来评估其疗效。