Sumi Chisato, Okamoto Akihisa, Tanaka Hiromasa, Nishi Kenichiro, Kusunoki Munenori, Shoji Tomohiro, Uba Takeo, Matsuo Yoshiyuki, Adachi Takehiko, Hayashi Jun-Ichi, Takenaga Keizo, Hirota Kiichi
Department of Anesthesiology, Kansai Medical University, Hirakata, Japan.
Department of Human Stress Response Science, Institute of Biomedical Science, Kansai Medical University, Hirakata, Japan.
PLoS One. 2018 Feb 15;13(2):e0192796. doi: 10.1371/journal.pone.0192796. eCollection 2018.
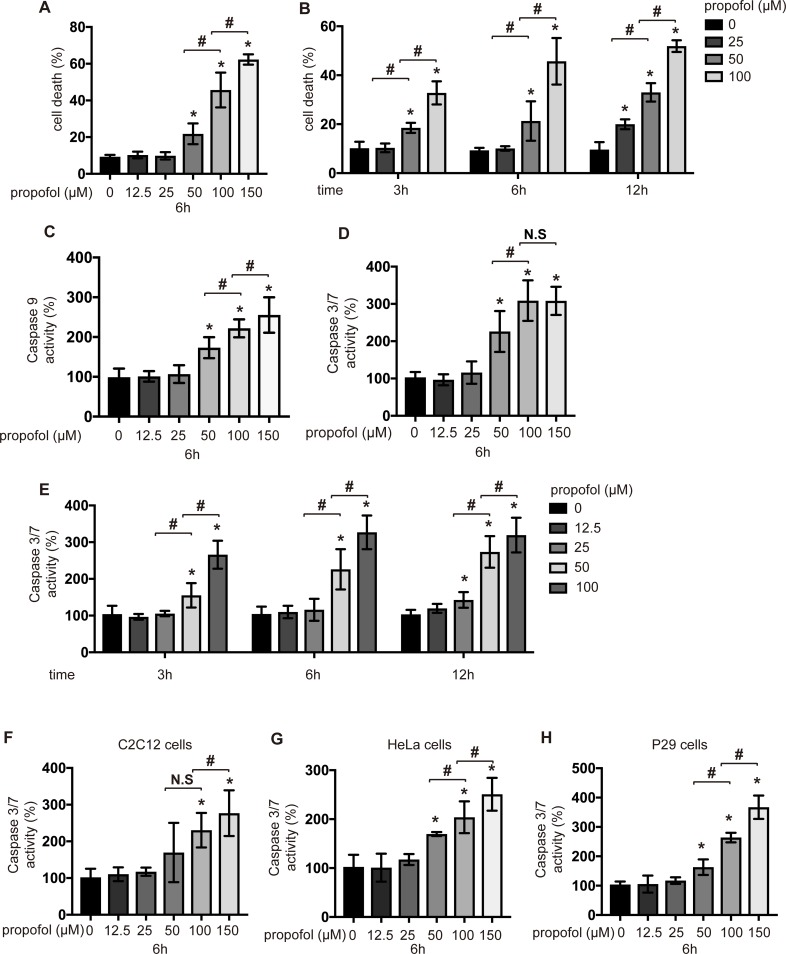
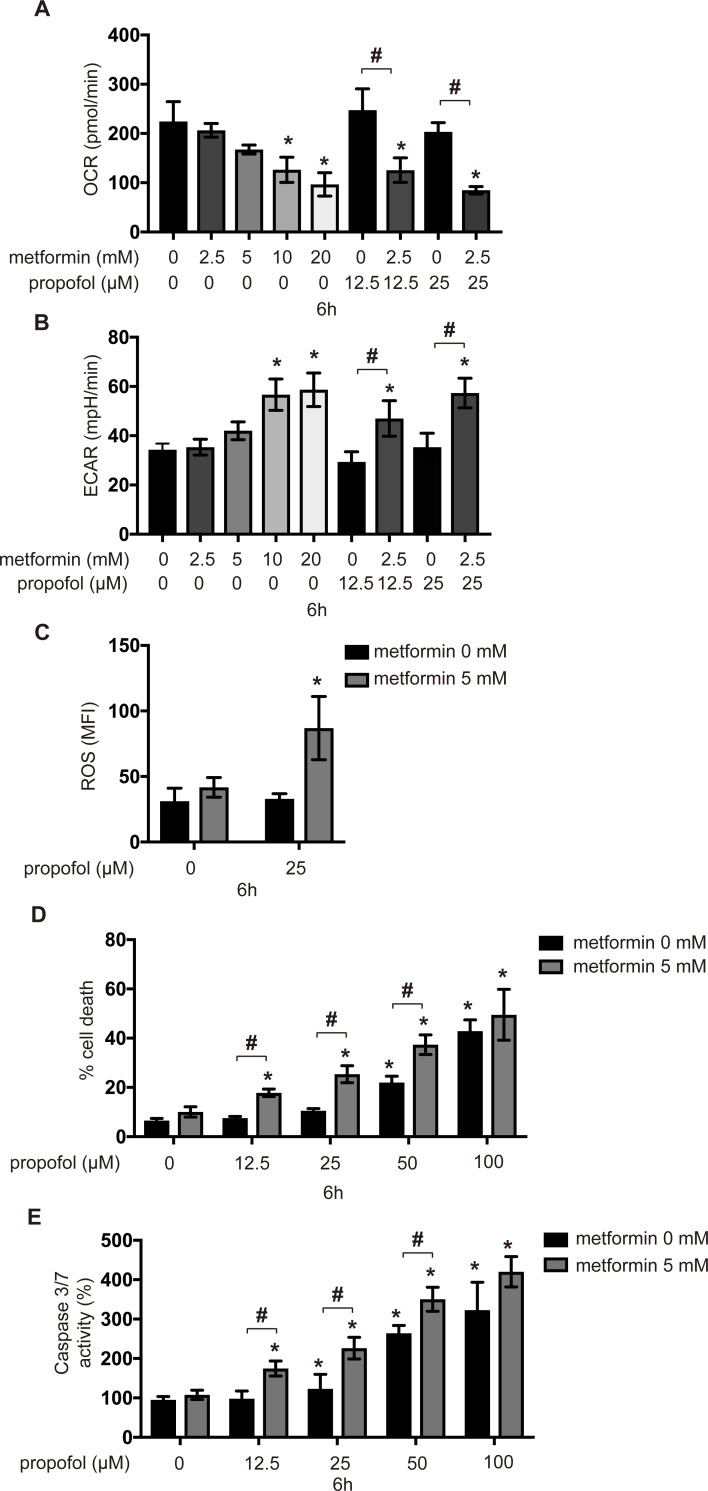
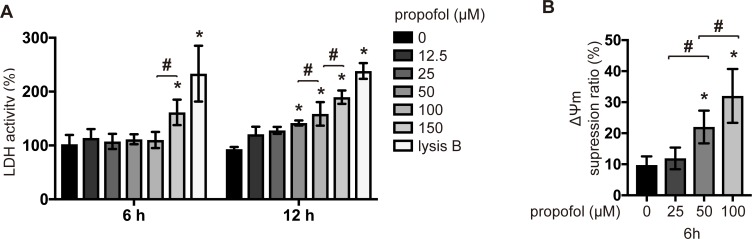
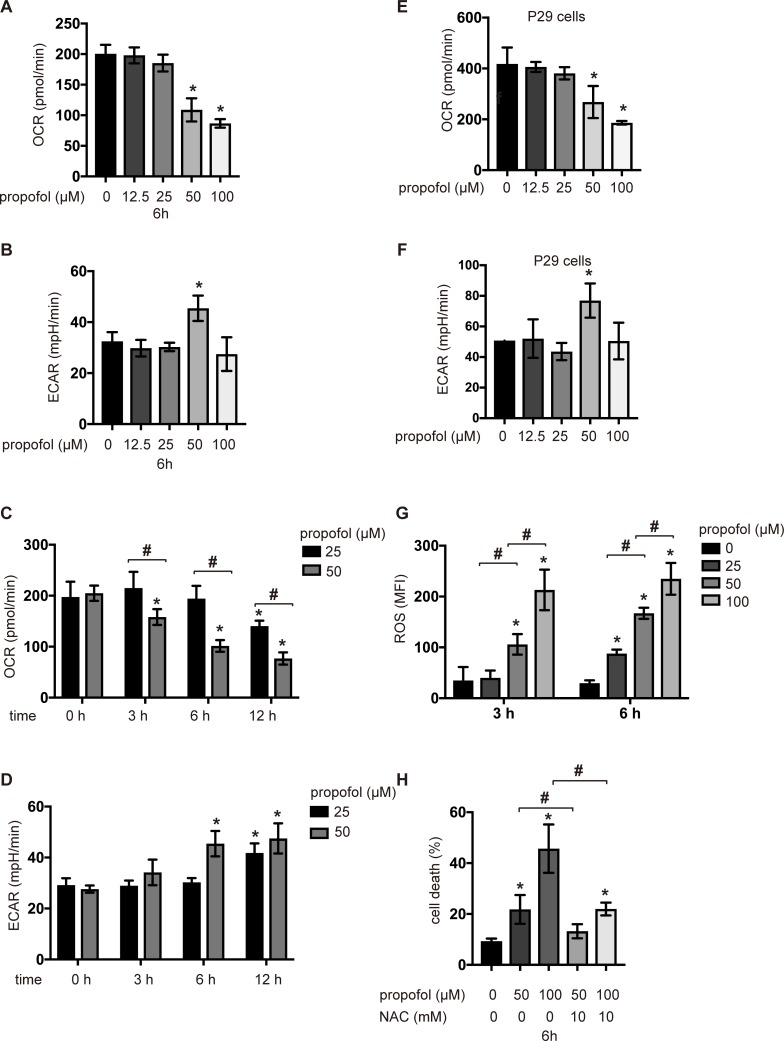
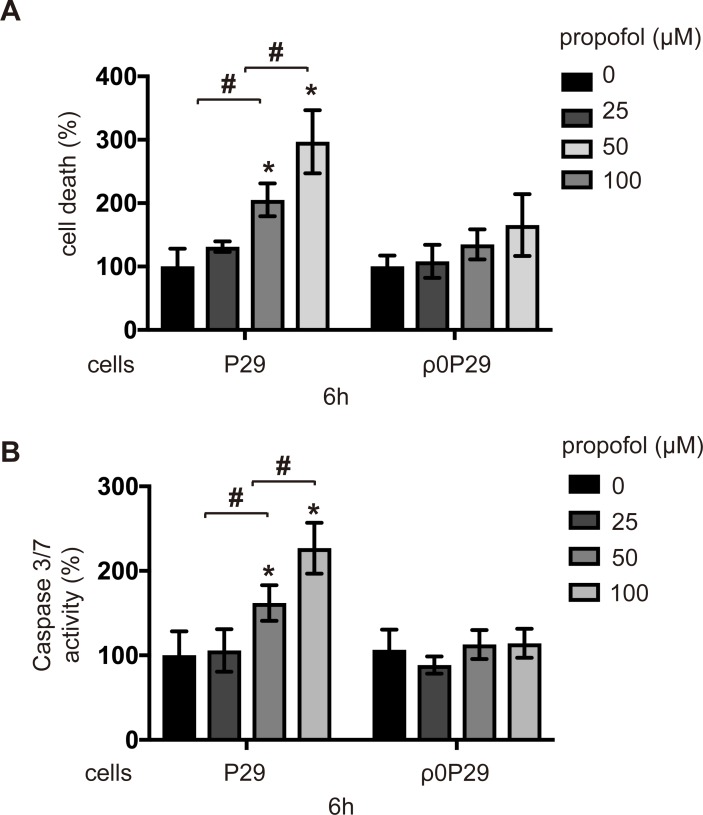
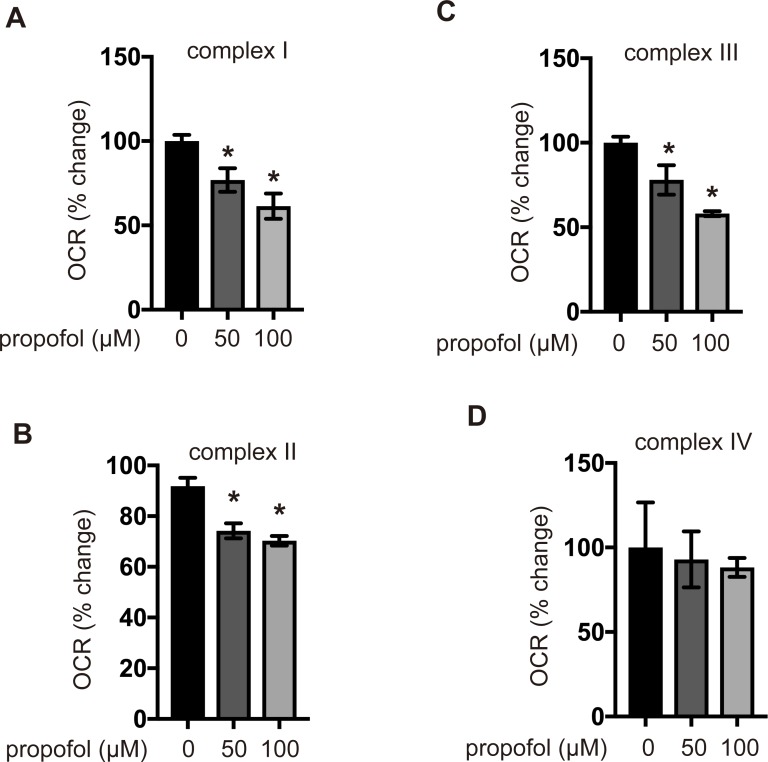
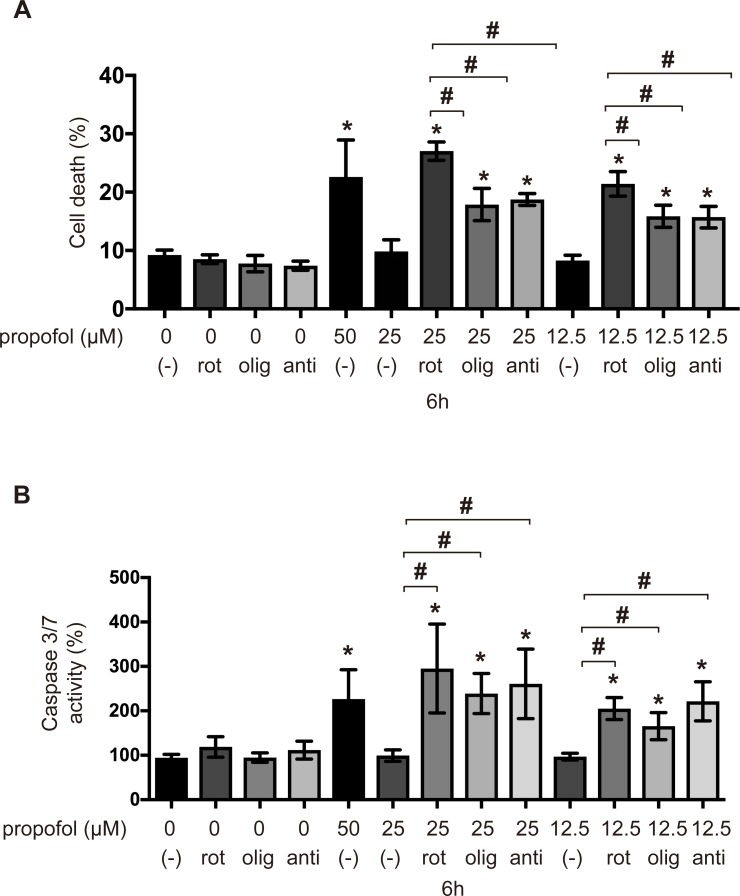
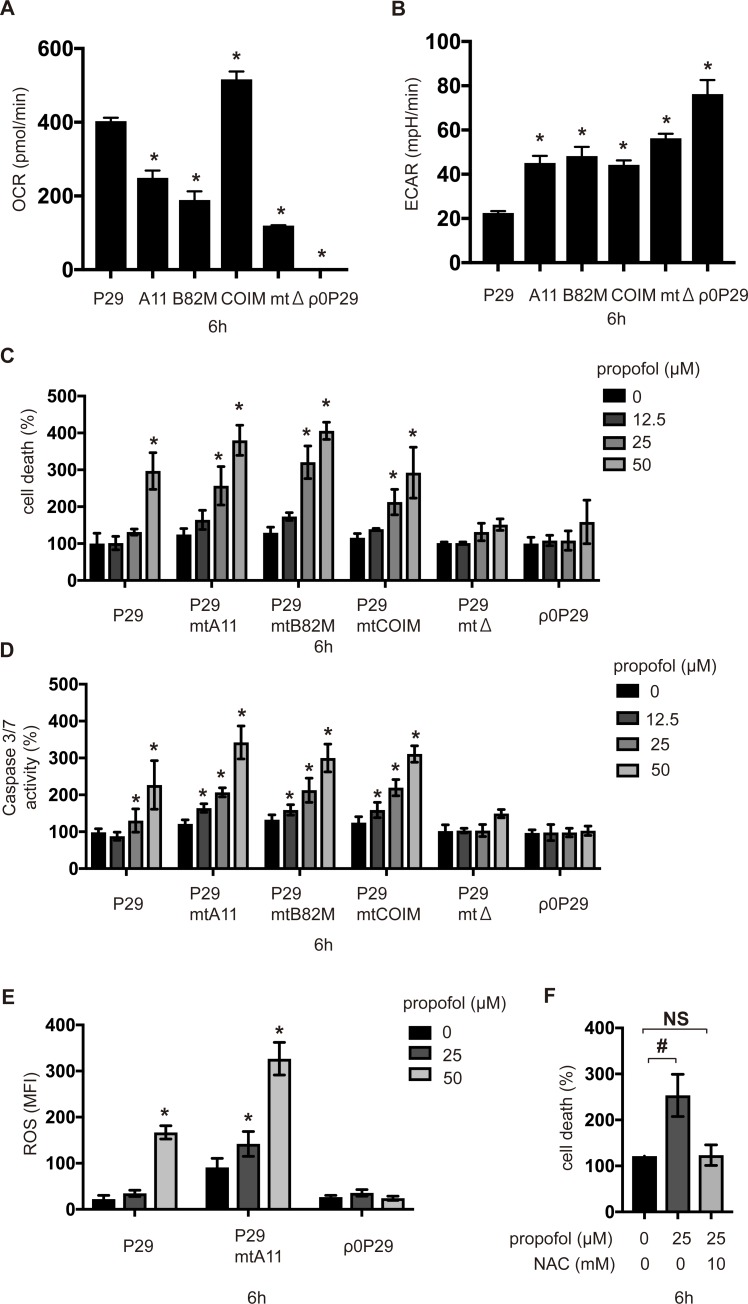
The intravenous anesthetic propofol (2,6-diisopropylphenol) has been used for the induction and maintenance of anesthesia and sedation in critical patient care. However, the rare but severe complication propofol infusion syndrome (PRIS) can occur, especially in patients receiving high doses of propofol for prolonged periods. In vivo and in vitro evidence suggests that the propofol toxicity is related to the impaired mitochondrial function. However, underlying molecular mechanisms remain unknown. Therefore, we investigated effects of propofol on cell metabolism and death using a series of established cell lines of various origins, including neurons, myocytes, and trans-mitochondrial cybrids, with defined mitochondrial DNA deficits. We demonstrated that supraclinical concentrations of propofol in not less than 50 μM disturbed the mitochondrial function and induced a metabolic switch, from oxidative phosphorylation to glycolysis, by targeting mitochondrial complexes I, II and III. This disturbance in mitochondrial electron transport caused the generation of reactive oxygen species, resulting in apoptosis. We also found that a predisposition to mitochondrial dysfunction, caused by a genetic mutation or pharmacological suppression of the electron transport chain by biguanides such as metformin and phenformin, promoted propofol-induced caspase activation and cell death induced by clinical relevant concentrations of propofol in not more than 25 μM. With further experiments with appropriate in vivo model, it is possible that the processes to constitute the molecular basis of PRIS are identified.
静脉麻醉药丙泊酚(2,6 - 二异丙基苯酚)已用于危重症患者的麻醉诱导和维持镇静。然而,可能会发生罕见但严重的并发症——丙泊酚输注综合征(PRIS),尤其是长时间接受高剂量丙泊酚的患者。体内和体外证据表明,丙泊酚毒性与线粒体功能受损有关。然而,其潜在的分子机制仍不清楚。因此,我们使用一系列已建立的不同来源的细胞系,包括神经元、心肌细胞和具有特定线粒体DNA缺陷的转线粒体杂交细胞,研究了丙泊酚对细胞代谢和死亡的影响。我们证明,临床超浓度的丙泊酚(不少于50μM)通过靶向线粒体复合物I、II和III,扰乱线粒体功能并诱导代谢转换,从氧化磷酸化转变为糖酵解。线粒体电子传递的这种紊乱导致活性氧的产生,从而导致细胞凋亡。我们还发现,由基因突变或二甲双胍和苯乙双胍等双胍类药物对电子传递链的药理学抑制引起的线粒体功能障碍易感性,促进了丙泊酚诱导的半胱天冬酶激活以及临床相关浓度(不超过25μM)的丙泊酚诱导的细胞死亡。通过使用合适的体内模型进行进一步实验,有可能确定构成PRIS分子基础的过程。