Kamal Sanaa, Aldossari Khaled K, Ghoraba Dhalia, Abdelhakam Sara Mahmoud, Kamal Amgad H, Bedewi Mohamad, Nabegh Leila, Bahnasy Khaled, Hafez Tamer
Department of Gastroenterology and Tropical Medicine, Ain Shams University Faculty of Medicine, Cairo, Egypt.
Department of Medicine, PSAU, Cairo, Egypt.
BMJ Open Gastroenterol. 2018 Jan 29;5(1):e000150. doi: 10.1136/bmjgast-2017-000150. eCollection 2018.
Concomitant non-alcoholic fatty liver disease (NAFLD) and coeliac disease (CD) have not been adequately studied. This study investigated the frequency of CD among NAFLD patients and the clinicopathological and immunological patterns and outcome of concomitant NAFLD and CD.
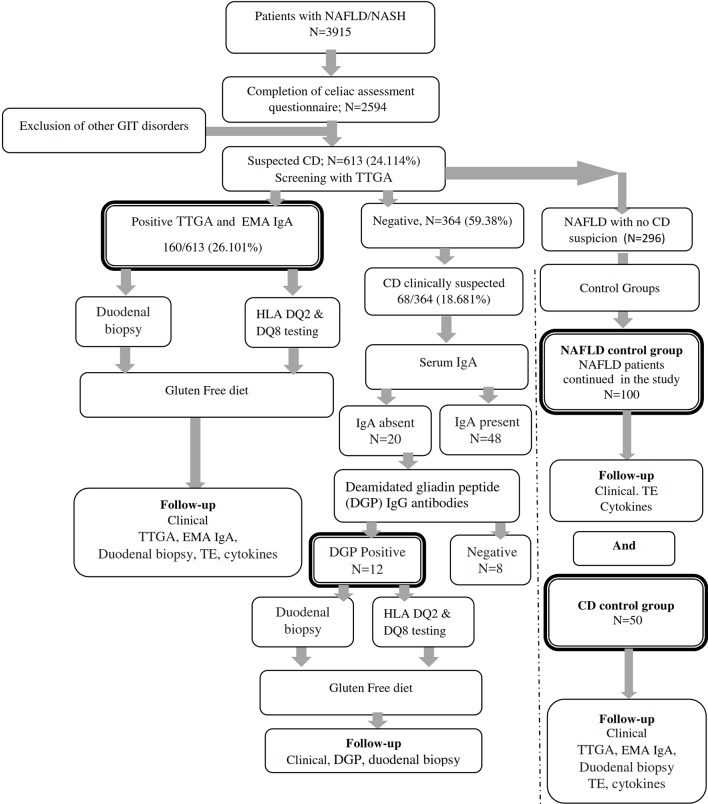
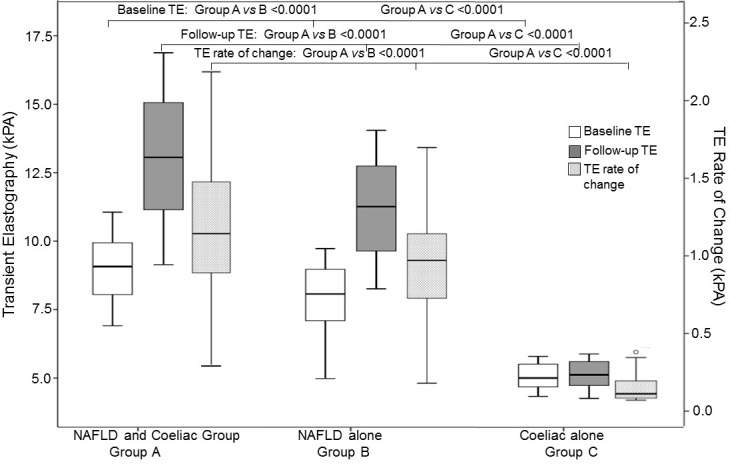
This prospective longitudinal study screened patients with NAFLD for CD (tissue transglutaminase antibodies (TTGA); anti-TTGA and antiendomysial antibodies (EMA)). Patients with concomitant NAFLD and CD and patients with either NAFLD or CD were enrolled and followed. Duodenal biopsy, transient elastography, tumour necrosis factor (TNF)-alpha, transforming growth factor-beta, interleukins (ILs) 1, 6, 10, 15 and 17, folic acid and vitamins B12 and D were performed at baseline and 1 year after gluten-free diet (GFD).
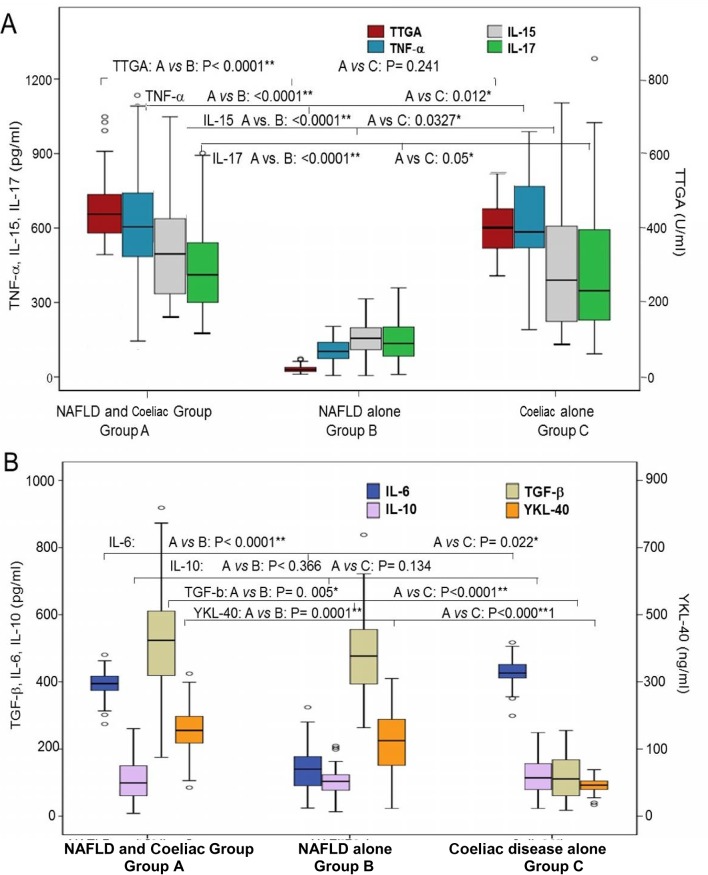
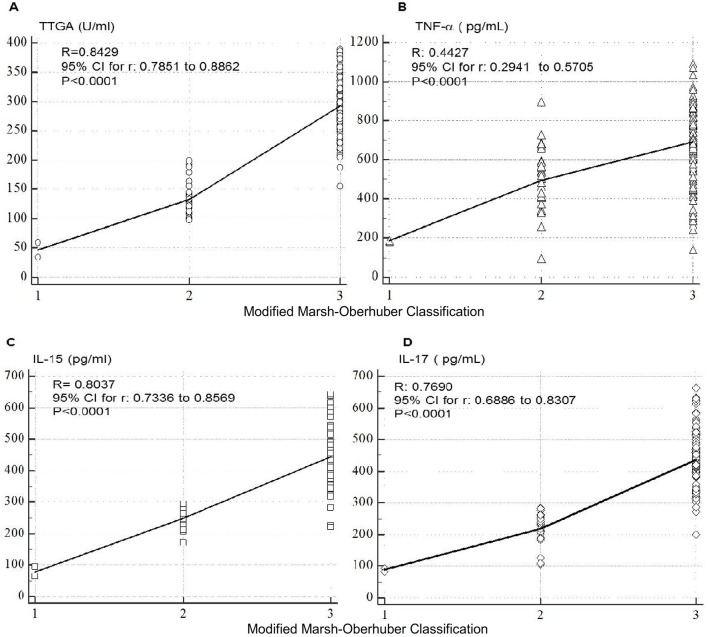
CD was confirmed in 7.2% of patients with NAFLD. Refractory anaemia and nutritional deficiencies were frequent in patients with concomitant NAFLD and CD who had advanced intestinal and hepatic lesions, higher levels of TNF-α, IL-15 and IL-17 compared with patients with CD and NAFLD. Patients concomittant CD and NAFLD showed clinical response to GFD, but intestinal histological improvement was suboptimal. Combining EMA-IgA or anti-TTGA with either IL-15 or IL-17 enhances the prognostic performance of both tests in predicting histological response to GFD.
Concomitant NAFLD and CD is not uncommon. Recurrent abdominal symptoms, refractory anaemia, nutritional deficiencies in patients with NAFLD warrant screening for CD. The study has important clinical implications since failure in diagnosing CD in patients with NAFLD patients results in marked intestinal and hepatic damage and suboptimal response to GFD that can be alleviated by early diagnosis and initiation of GFD.
非酒精性脂肪性肝病(NAFLD)与乳糜泻(CD)并存的情况尚未得到充分研究。本研究调查了NAFLD患者中CD的发生率,以及NAFLD与CD并存时的临床病理、免疫学模式及转归。
这项前瞻性纵向研究对NAFLD患者进行CD筛查(组织转谷氨酰胺酶抗体(TTGA);抗TTGA和抗肌内膜抗体(EMA))。纳入NAFLD与CD并存的患者以及单独患有NAFLD或CD的患者并进行随访。在基线时以及无谷蛋白饮食(GFD)1年后进行十二指肠活检、瞬时弹性成像、肿瘤坏死因子(TNF)-α、转化生长因子-β、白细胞介素(ILs)1、6、10、15和17、叶酸以及维生素B12和D检测。
7.2%的NAFLD患者确诊患有CD。与单独患有CD和NAFLD的患者相比,NAFLD与CD并存且伴有晚期肠道和肝脏病变的患者中难治性贫血和营养缺乏较为常见,其TNF-α、IL-15和IL-17水平更高。NAFLD与CD并存的患者对GFD有临床反应,但肠道组织学改善并不理想。将EMA-IgA或抗TTGA与IL-15或IL-17联合使用可提高这两种检测在预测对GFD组织学反应方面的预后性能。
NAFLD与CD并存并不罕见。NAFLD患者出现反复腹痛症状、难治性贫血和营养缺乏时,有必要筛查CD。该研究具有重要的临床意义,因为未能诊断出NAFLD患者中的CD会导致明显的肠道和肝脏损害以及对GFD的反应不佳,而早期诊断和开始GFD治疗可缓解这种情况。