Albion Centre, South Eastern Sydney Local Health District, Sydney, NSW, 2010, Australia.
School of Public Health and Community Medicine, Faculty of Medicine, University of New South Wales, Sydney, NSW, 2052, Australia.
AIDS Res Ther. 2018 Mar 8;15(1):6. doi: 10.1186/s12981-018-0193-z.
To assess the prevalence of non-AIDS co-morbidities (NACs) and predictors of adverse health outcomes amongst people living with HIV in order to identify health needs and potential gaps in patient management.
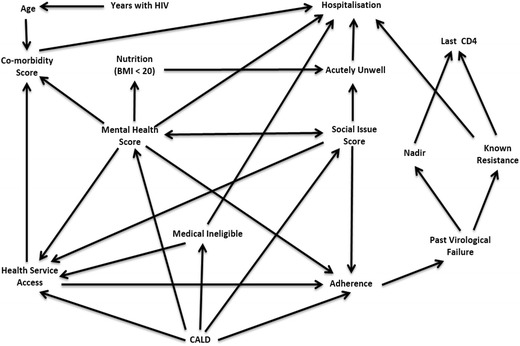
Retrospective, non-consecutive medical record audit of patients attending a publicly funded HIV clinic in metropolitan Sydney analysed for predictors of adverse health outcomes. We developed a scoring system based on the validated Charlson score method for NACs, mental health and social issues and confounders were selected using directed acyclic graph theory under the principles of causal inference.
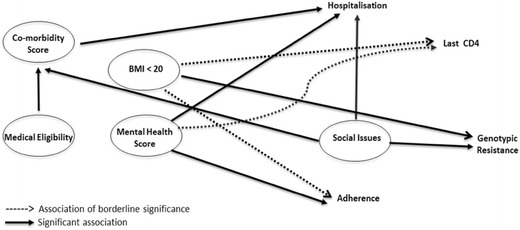
211 patient files were audited non-consecutively over 6 weeks. 89.5% were male; 41.8% culturally and linguistically diverse and 4.1% were of Aboriginal/Torres Strait Islander origin. Half of patients had no general practitioner and 25% were ineligible for Medicare subsidised care. The most common NACs were: cardiovascular disease (25%), hepatic disease (21%), and endocrinopathies (20%). One-third of patients had clinical anxiety, one-third major depression and almost half of patients had a lifetime history of tobacco smoking. Five predictors of poor health outcomes were identified: (1) co-morbidity score was associated with hospitalisation (odds ratio, OR 1.58; 95% CI 1.01-2.46; p = 0.044); (2) mental health score was associated with hospitalisation (OR 1.79; 95% CI 1.22-2.62; p = 0.003) and poor adherence to ART (OR 2.34; 95% CI 1.52-3.59; p = 0.001); (3) social issues score was associated with genotypic resistance (OR 2.61; 95% CI 1.48-4.59; p = 0.001), co-morbidity score (OR 1.69; 95% CI 1.24-2.3; p = 0.001) and hospitalisation (OR 1.72; 95% CI 1.1-2.7; p = 0.018); (4) body mass index < 20 was associated with genotypic resistance (OR 6.25; 95% CI 1.49-26.24; p = 0.012); and (5) Medicare eligibility was associated with co-morbidity score (OR 2.21; 95% CI 1.24-3.95; p = 0.007).
Most HIV patients are healthy due to effective antiretroviral therapy; however, NACs and social/mental health issues are adding to patient complexity. The current findings underpin the need for multidisciplinary management beyond routine viral load and CD4 count monitoring.
评估艾滋病毒感染者中非艾滋病合并症(NACs)的流行情况和不良健康结局的预测因素,以确定患者的健康需求和潜在的管理差距。
对在悉尼大都市一家公立艾滋病毒诊所就诊的患者进行回顾性、非连续的病历审核,以分析不良健康结局的预测因素。我们根据经过验证的 Charlson 评分方法为 NACs、心理健康和社会问题制定了评分系统,并根据因果推理原则使用有向无环图理论选择混杂因素。
在 6 周内非连续审核了 211 份患者档案。89.5%为男性;41.8%为文化和语言多样化,4.1%为原住民/托雷斯海峡岛民。一半的患者没有全科医生,25%的患者不符合医疗保险补贴护理的条件。最常见的 NACs 是:心血管疾病(25%)、肝脏疾病(21%)和内分泌疾病(20%)。三分之一的患者有临床焦虑,三分之一有重度抑郁症,近一半的患者有吸烟史。确定了 5 个不良健康结局的预测因素:(1)共病评分与住院有关(优势比,OR 1.58;95%CI 1.01-2.46;p=0.044);(2)心理健康评分与住院(OR 1.79;95%CI 1.22-2.62;p=0.003)和抗逆转录病毒治疗依从性差(OR 2.34;95%CI 1.52-3.59;p=0.001)有关;(3)社会问题评分与基因耐药性(OR 2.61;95%CI 1.48-4.59;p=0.001)、共病评分(OR 1.69;95%CI 1.24-2.3;p=0.001)和住院(OR 1.72;95%CI 1.1-2.7;p=0.018)有关;(4)BMI<20 与基因耐药性有关(OR 6.25;95%CI 1.49-26.24;p=0.012);(5)医疗保险资格与共病评分有关(OR 2.21;95%CI 1.24-3.95;p=0.007)。
由于有效的抗逆转录病毒治疗,大多数艾滋病毒感染者都很健康;然而,NACs 和社会/心理健康问题增加了患者的复杂性。目前的发现强调了需要进行多学科管理,而不仅仅是常规的病毒载量和 CD4 计数监测。