University Institute of Family Medicine, Department of Ambulatory Care and Community Medicine (DACCM), University of Lausanne, Rue du Bugnon 44, 1011, Lausanne, Switzerland.
Public Health Office of the Canton of Vaud, Av. des casernes 2, 1014, Lausanne, Switzerland.
BMC Geriatr. 2018 Mar 13;18(1):72. doi: 10.1186/s12877-018-0761-z.
Geriatric syndromes are rarely detected in family medicine. Within the AGE program (active geriatric evaluation), a brief assessment tool (BAT) designed for family physicians (FP) was developed and its diagnostic performance estimated by comparison to a comprehensive geriatric assessment.
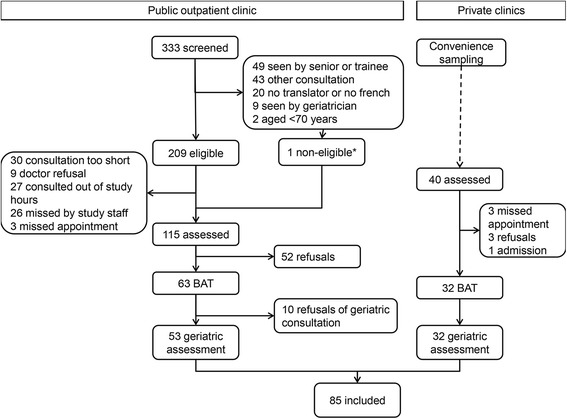
This prospective diagnostic study was conducted in four primary care sites in Switzerland. Participants were aged at least 70 years and attending a routine appointment with their physician, without previous documented geriatric assessment. Participants were assessed by their family physicians using the BAT, and by a geriatriciant who performed a comprehensive geriatric assessment within the following two-month period (reference standard). Both the BAT and the full assessment targeted eight geriatric syndromes: cognitive impairment, mood impairment, urinary incontinence, visual impairment, hearing loss, undernutrition, osteoporosis and gait and balance impairment. Diagnostic accuracy of the BAT was estimated in terms of sensitivity, specificity, and predictive values; secondary outcomes were measures of feasibility, in terms of added consultation time and comprehensiveness in applying the BAT items.
Prevalence of the geriatric syndromes in participants (N=85, 46 (54.1%) women, mean age 78 years (SD 6))ranged from 30.0% (malnutrition and cognitive impairment) to 71.0% (visual impairment), with a median number of 3 syndromes (IQR 2 to 4) per participant. Sensitivity of the BAT ranged from 25.0% for undernutrition (95%CI 9.8% - 46.7%) to 82.1% for hearing impairment (95%CI 66.5% - 92.5%), while specificity ranged from 45.8% for visual impairment (95%CI 25.6-67.2) to 87.7% for undernutrition (76.3% to 94.9%). Finally, most negative predictive values (NPV) were between 73.5% and 84.1%, excluding visual impairment with a NPV of 50.0%. Family physicians reported BAT use as per instructions for 76.7% of the syndromes assessed.
Although the BAT does not replace a comprehensive geriatric assessment, it is a useful and appropriate tool for the FP to screen elderly patients for most geriatric syndromes.
The study was registered on ClinicalTrials.gov on February 20, 2013 ( NCT01816087 ).
老年综合征在家庭医学中很少被发现。在 AGE 计划(积极老年评估)中,为家庭医生设计了一种简短的评估工具(BAT),并通过与全面老年评估的比较来估计其诊断性能。
这项前瞻性诊断研究在瑞士的四个初级保健点进行。参与者年龄至少为 70 岁,正在与他们的医生进行常规预约,之前没有记录过老年评估。参与者由他们的家庭医生使用 BAT 进行评估,并由一名老年病学家在接下来的两个月内进行全面的老年评估(参考标准)。BAT 和完整评估都针对八种老年综合征:认知障碍、情绪障碍、尿失禁、视力障碍、听力损失、营养不良、骨质疏松症和步态及平衡障碍。BAT 的诊断准确性以敏感性、特异性和预测值来衡量;次要结果是衡量可行性的措施,包括咨询时间的增加和应用 BAT 项目的全面性。
参与者(N=85,46 名女性,平均年龄 78 岁(SD 6))中老年综合征的患病率范围为 30.0%(营养不良和认知障碍)至 71.0%(视力障碍),中位数为 3 个综合征(IQR 2 至 4)/参与者。BAT 的敏感性范围为 25.0%(营养不良)(95%CI 9.8% - 46.7%)至 82.1%(听力损失)(95%CI 66.5% - 92.5%),而特异性范围为 45.8%(视力障碍)(95%CI 25.6-67.2)至 87.7%(营养不良)(76.3%至 94.9%)。最后,大多数阴性预测值(NPV)在 73.5%至 84.1%之间,不包括视力障碍的 NPV 为 50.0%。家庭医生报告说,他们按照指令使用 BAT 评估了 76.7%的综合征。
尽管 BAT 不能替代全面的老年评估,但它是家庭医生筛查老年患者大多数老年综合征的有用和适当的工具。
该研究于 2013 年 2 月 20 日在 ClinicalTrials.gov 上注册(NCT01816087)。