Department of Primary Care and Public Health, Brighton and Sussex Medical School, Brighton, United Kingdom.
Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore.
PLoS One. 2018 Mar 29;13(3):e0194735. doi: 10.1371/journal.pone.0194735. eCollection 2018.
Possible dementia is usually identified in primary care by general practitioners (GPs) who refer to specialists for diagnosis. Only two-thirds of dementia cases are currently recorded in primary care, so increasing the proportion of cases diagnosed is a strategic priority for the UK and internationally. Variables in the primary care record may indicate risk of developing dementia, and could be combined in a predictive model to help find patients who are missing a diagnosis. We conducted a meta-analysis to identify clinical entities with potential for use in such a predictive model for dementia in primary care.
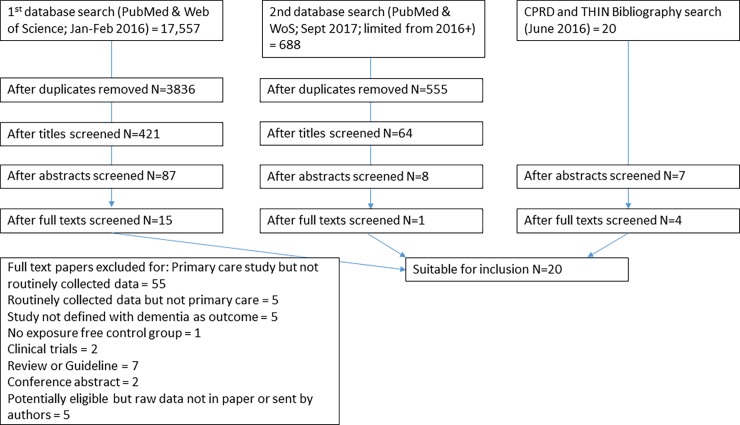
We conducted a systematic search in PubMed, Web of Science and primary care database bibliographies. We included cohort or case-control studies which used routinely collected primary care data, to measure the association between any clinical entity and dementia. Meta-analyses were performed to pool odds ratios. A sensitivity analysis assessed the impact of non-independence of cases between studies. From a sift of 3836 papers, 20 studies, all European, were eligible for inclusion, comprising >1 million patients. 75 clinical entities were assessed as risk factors for all cause dementia, Alzheimer's (AD) and Vascular dementia (VaD). Data included were unexpectedly heterogeneous, and assumptions were made about definitions of clinical entities and timing as these were not all well described. Meta-analysis showed that neuropsychiatric symptoms including depression, anxiety, and seizures, cognitive symptoms, and history of stroke, were positively associated with dementia. Cardiovascular risk factors such as hypertension, heart disease, dyslipidaemia and diabetes were positively associated with VaD and negatively with AD. Sensitivity analyses showed similar results.
These findings are of potential value in guiding feature selection for a risk prediction tool for dementia in primary care. Limitations include findings being UK-focussed. Further predictive entities ascertainable from primary care data, such as changes in consulting patterns, were absent from the literature and should also be explored in future studies.
初级保健医生(全科医生)通常通过初级保健识别可能的痴呆症患者,并将其转介给专家进行诊断。目前只有三分之二的痴呆症病例在初级保健中记录,因此增加诊断病例的比例是英国和国际上的战略重点。初级保健记录中的变量可能表明发展为痴呆症的风险,并且可以组合在预测模型中,以帮助发现漏诊的患者。我们进行了一项荟萃分析,以确定在初级保健中用于预测痴呆症的潜在临床实体。
我们在 PubMed、Web of Science 和初级保健数据库书目进行了系统搜索。我们纳入了使用常规收集的初级保健数据来衡量任何临床实体与痴呆症之间关联的队列或病例对照研究。进行了荟萃分析以汇总优势比。敏感性分析评估了研究之间病例非独立性的影响。从 3836 篇论文中筛选出 20 项研究,这些研究均来自欧洲,符合纳入标准,共纳入>100 万名患者。评估了 75 种临床实体作为所有原因痴呆、阿尔茨海默病(AD)和血管性痴呆(VaD)的危险因素。数据出乎意料地存在异质性,并且对临床实体的定义和时间的假设是基于这些定义和时间没有被很好地描述。荟萃分析表明,神经精神症状(包括抑郁、焦虑和癫痫发作)、认知症状和中风史与痴呆症呈正相关。心血管危险因素(如高血压、心脏病、血脂异常和糖尿病)与 VaD 呈正相关,与 AD 呈负相关。敏感性分析显示出类似的结果。
这些发现对于指导初级保健中痴呆症风险预测工具的特征选择具有潜在价值。局限性包括研究结果仅针对英国。进一步可从初级保健数据中确定的预测实体,如咨询模式的变化,在文献中不存在,也应在未来的研究中探索。