SUNY Upstate Medical University, Syracuse, NY, United States.
Alliance Statistics and Data Center, Duke University Medical Center, Durham, NC, United States.
J Geriatr Oncol. 2018 May;9(3):221-227. doi: 10.1016/j.jgo.2018.02.003. Epub 2018 Mar 28.
Chemotherapy preference refers to a patient's interest in receiving chemotherapy. This study examined whether chemotherapy preference was associated with toxicity, efficacy, quality of life (QoL), and functional outcomes during and after completion of adjuvant chemotherapy in older women with breast cancer.
This study is a secondary analysis of CALGB 49907, a randomized trial that compared standard adjuvant chemotherapy versus capecitabine in patients age 65 years or older with breast cancer. A subset of 145 patients completed a questionnaire to describe chemotherapy preference pre-treatment. The association of this pre-treatment preference with the patient's perception of self-health, predicted and actual QoL, patient- and professional-reported toxicity, mental health, self-rated function, and survival was studied during and after treatment.
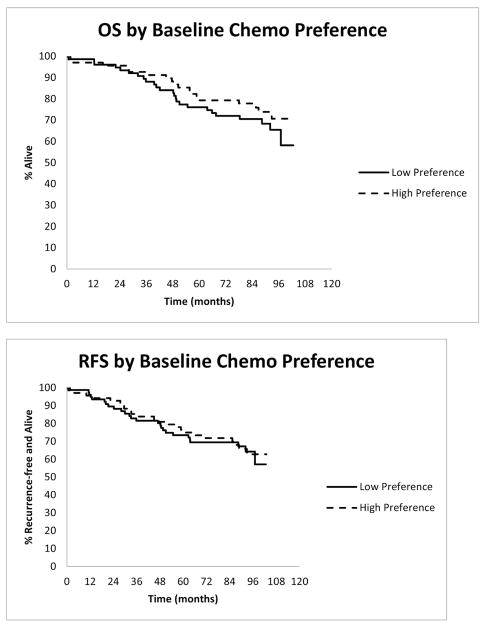
The median age of patients was 71 years and 47% had a high preference for chemotherapy. On baseline demographics, the low preference group had a higher proportion of white patients (95% vs. 78%, p = 0.004). Before treatment, low chemotherapy preference was associated with greater nausea/vomiting (p = 0.008). Mid-treatment, low preference was associated with lower QoL, worse social, emotional and physical function (all p ≤ 0.02) and worse nausea/vomiting, cancer symptoms and financial worries (all p < 0.05). The association noted mid-treatment, resolved after treatment completion except with financial worries which persisted at 24 months. Low preference was associated with higher rates of grade 3-5 adverse events (53% vs. 34%, p = 0.02) but was not associated with survival.
Low chemotherapy preference prior to treatment initiation was associated with lower QoL, worse physical symptoms and self-rated function and more adverse events mid-treatment. There is no association of chemotherapy preference with survival.
化疗偏好是指患者对接受化疗的兴趣。本研究旨在探讨化疗偏好是否与毒性、疗效、生活质量(QoL)以及老年乳腺癌患者辅助化疗期间和完成后的功能结局相关。
本研究是 CALGB 49907 的二次分析,该随机试验比较了标准辅助化疗与卡培他滨在 65 岁及以上乳腺癌患者中的疗效。有 145 例患者完成了一份问卷,以描述治疗前的化疗偏好。在治疗期间和治疗后,研究了这种治疗前偏好与患者自我健康感知、预测和实际 QoL、患者和专业人员报告的毒性、心理健康、自我评定功能以及生存之间的关系。
患者的中位年龄为 71 岁,47%的患者对化疗有强烈的偏好。在基线人口统计学方面,低化疗偏好组的白人患者比例较高(95% vs. 78%,p=0.004)。在治疗前,低化疗偏好与更高的恶心/呕吐发生率相关(p=0.008)。在治疗中期,低化疗偏好与较低的 QoL、较差的社会、情感和身体功能相关(所有 p 值均≤0.02),以及更严重的恶心/呕吐、癌症症状和经济担忧(所有 p 值均<0.05)相关。这些关联在治疗结束后得到缓解,但在 24 个月时,经济担忧仍存在。低化疗偏好与较高的 3-5 级不良事件发生率相关(53% vs. 34%,p=0.02),但与生存无关。
在开始治疗前,低化疗偏好与治疗中期较低的 QoL、更严重的身体症状和自我评定功能以及更多的不良事件相关。化疗偏好与生存无关。