Rosumeck Stefanie, Nast Alexander, Dressler Corinna
Division of Evidence Based Medicine, Department of Dermatology, Venerology and Allergology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Charitéplatz 1, Berlin, Berlin, Germany, 10117.
Cochrane Database Syst Rev. 2018 Apr 2;4(4):CD012994. doi: 10.1002/14651858.CD012994.
Scabies is an intensely itchy parasitic infection of the skin. It occurs worldwide, but is particularly problematic in areas of poor sanitation, overcrowding, and social disruption. In recent years, permethrin and ivermectin have become the most relevant treatment options for scabies.
To assess the efficacy and safety of topical permethrin and topical or systemic ivermectin for scabies in people of all ages.
We searched the following databases up to 25 April 2017: the Cochrane Infectious Diseases Group Specialized Register, CENTRAL, MEDLINE, Embase, LILACS, and IndMED. We searched the World Health Organization International Clinical Trials Registry Platform, the ISRCTN registry, CenterWatch Clinical Trials Listing, ClinicalTrials.gov, TrialsCentral, and the UK Department of Health National Research Register for ongoing trials. We also searched multiple sources for grey literature and checked reference lists of included studies for additional trials.
We included randomized controlled trials that compared permethrin or ivermectin against each other for people with scabies of all ages and either sex.
Two review authors independently screened the identified records, extracted data, and assessed the risk of bias for the included trials.The primary outcome was complete clearance of scabies. Secondary outcomes were number of participants re-treated, number of participants with at least one adverse event, and number of participants withdrawn from study due to an adverse event.We summarized dichotomous outcomes using risk ratios (RR) with 95% confidence intervals (CI). If it was not possible to calculate the point estimate, we described the data qualitatively. Where appropriate, we calculated combined effect estimates using a random-effects model and assessed heterogeneity. We calculated numbers needed to treat for an additional beneficial outcome when we found a difference.We assessed the certainty of the evidence using the GRADE approach. We used the control rate average to provide illustrative clearance rates in the comparison groups.
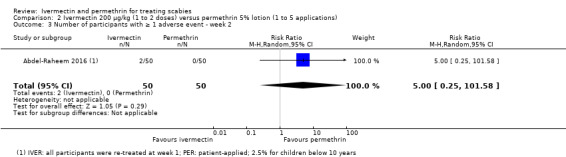
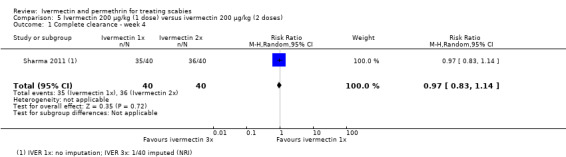
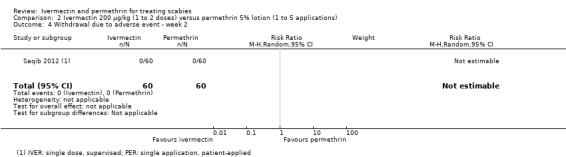
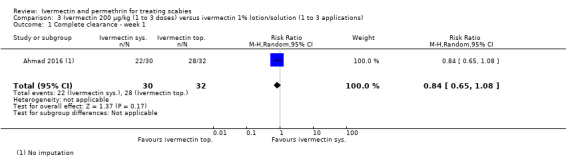
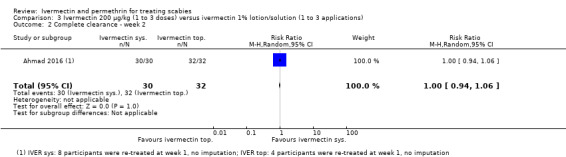
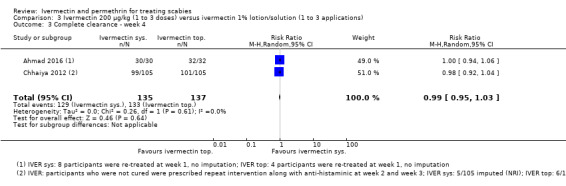
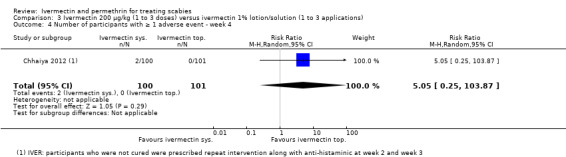
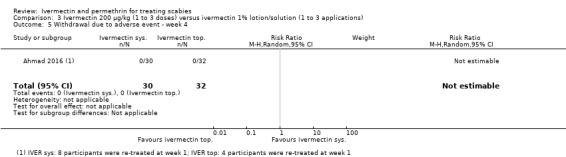
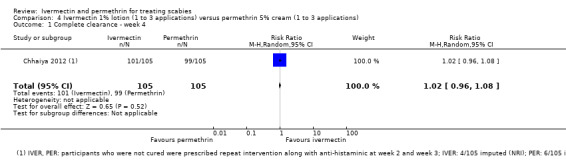
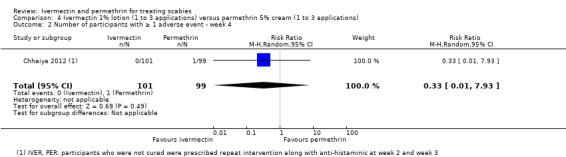
Fifteen studies (1896 participants) comparing topical permethrin, systemic ivermectin, or topical ivermectin met the inclusion criteria. Overall, the risk of bias in the included trials was moderate: reporting in many studies was poor. Nearly all studies were conducted in South Asia or North Africa, where the disease is more common, and is associated with poverty.EfficacyOral ivermectin (at a standard dose of 200 μg/kg) may lead to slightly lower rates of complete clearance after one week compared to permethrin 5% cream. Using the average clearance rate of 65% in the trials with permethrin, the illustrative clearance with ivermectin is 43% (RR 0.65, 95% CI 0.54 to 0.78; 613 participants, 6 studies; low-certainty evidence). However, by week two there may be little or no difference (illustrative clearance of permethrin 74% compared to ivermectin 68%; RR 0.91, 95% CI 0.76 to 1.08; 459 participants, 5 studies; low-certainty evidence). Treatments with one to three doses of ivermectin or one to three applications of permethrin may lead to little or no difference in rates of complete clearance after four weeks' follow-up (illustrative cures with 1 to 3 applications of permethrin 93% and with 1 to 3 doses of ivermectin 86%; RR 0.92, 95% CI 0.82 to 1.03; 581 participants, 5 studies; low-certainty evidence).After one week of treatment with oral ivermectin at a standard dose of 200 μg/kg or one application of permethrin 5% lotion, there is probably little or no difference in complete clearance rates (illustrative cure rates: permethrin 73%, ivermectin 68%; RR 0.93, 95% CI 0.74 to 1.17; 120 participants, 1 study; moderate-certainty evidence). After two weeks of treatment, one dose of systemic ivermectin compared to one application of permethrin lotion may lead to similar complete clearance rates (extrapolated cure rates: 67% in both groups; RR 1.00, 95% CI 0.78 to 1.29; 120 participants, 1 study; low-certainty evidence).There is probably little or no difference in rates of complete clearance between systemic ivermectin at standard dose and topical ivermectin 1% lotion four weeks after initiation of treatment (illustrative cure rates: oral ivermectin 97%, ivermectin lotion 96%; RR 0.99, 95% CI 0.95 to 1.03; 272 participants, 2 studies; moderate-certainty evidence). Likewise, after four weeks, ivermectin lotion probably leads to little or no difference in rates of complete clearance when compared to permethrin cream (extrapolated cure rates: permethrin cream 94%, ivermectin lotion 96%; RR 1.02, 95% CI 0.96 to 1.08; 210 participants, 1 study; moderate-certainty evidence), and there is little or no difference among systemic ivermectin in different doses (extrapolated cure rates: 2 doses 90%, 1 dose 87%; RR 0.97, 95% CI 0.83 to 1.14; 80 participants, 1 study; high-certainty evidence).SafetyReporting of adverse events in the included studies was suboptimal. No withdrawals due to adverse events occurred in either the systemic ivermectin or the permethrin group (moderate-certainty evidence). Two weeks after treatment initiation, there is probably little or no difference in the proportion of participants treated with systemic ivermectin or permethrin cream who experienced at least one adverse event (55 participants, 1 study; moderate-certainty evidence). After four weeks, ivermectin may lead to a slightly larger proportion of participants with at least one adverse event (extrapolated rates: permethrin 4%, ivermectin 5%; RR 1.30, 95% CI 0.35 to 4.83; 502 participants, 4 studies; low-certainty evidence).Adverse events in participants treated with topical ivermectin were rare and of mild intensity and comparable to those with systemic ivermectin. For this comparison, it is uncertain whether there is any difference in the number of participants with at least one adverse event (very low-certainty evidence). No withdrawals due to adverse events occurred (62 participants, 1 study; moderate-certainty evidence).It is uncertain whether topical ivermectin or permethrin differ in the number of participants with at least one adverse event (very low-certainty evidence). We found no studies comparing systemic ivermectin in different doses that assessed safety outcomes.
AUTHORS' CONCLUSIONS: We found that for the most part, there was no difference detected in the efficacy of permethrin compared to systemic or topical ivermectin. Overall, few and mild adverse events were reported. Our confidence in the effect estimates was mostly low to moderate. Poor reporting is a major limitation.
疥疮是一种引起强烈瘙痒的皮肤寄生虫感染。该病在全球范围内均有发生,但在卫生条件差、过度拥挤和社会动荡的地区问题尤为突出。近年来,氯菊酯和伊维菌素已成为治疗疥疮最常用的药物。
评估外用氯菊酯以及外用或全身性伊维菌素治疗各年龄段人群疥疮的疗效和安全性。
截至2017年4月25日,我们检索了以下数据库:Cochrane传染病专业组注册库、Cochrane系统评价数据库、医学期刊数据库、荷兰医学文摘数据库、拉丁美洲和加勒比地区卫生科学数据库以及印度医学数据库。我们检索了世界卫生组织国际临床试验注册平台、国际标准随机对照试验编号注册库、CenterWatch临床试验列表、美国国立医学图书馆临床试验数据库、TrialsCentral以及英国卫生部国家研究注册库以查找正在进行的试验。我们还通过多种渠道检索灰色文献,并查阅纳入研究的参考文献列表以寻找其他试验。
我们纳入了比较氯菊酯或伊维菌素治疗各年龄段、不同性别的疥疮患者疗效的随机对照试验。
两名综述作者独立筛选识别出的记录,并提取数据,同时评估纳入试验中的偏倚风险。主要结局为疥疮完全清除。次要结局为再次接受治疗的参与者数量、至少发生1起不良事件的参与者数量以及因不良事件退出研究的参与者数量。我们采用风险比(RR)及95%置信区间(CI)总结二分法结局。若无法计算点估计值,我们将对数据进行定性描述。在适当情况下,我们采用随机效应模型计算合并效应估计值并评估异质性。当发现差异时,我们计算获得额外有益结局所需的治疗人数。我们采用GRADE方法评估证据的确定性。我们使用对照组平均清除率来展示比较组中的清除率。
15项比较外用氯菊酯、全身性伊维菌素或外用伊维菌素的研究(1896名参与者)符合纳入标准。总体而言,纳入试验中的偏倚风险为中度:许多研究报告质量较差。几乎所有研究均在南亚或北非进行,这些地区该病更为常见,且与贫困相关。
口服伊维菌素(标准剂量200μg/kg)与5%氯菊酯乳膏相比,治疗1周后可能导致完全清除率略低。在使用氯菊酯的试验中,平均清除率为65%,伊维菌素的预估清除率为43%(RR 0.65,95%CI 0.54至0.78;613名参与者,6项研究;低确定性证据)。然而,到第2周时可能几乎没有差异(氯菊酯预估清除率为74%,伊维菌素为68%;RR 0.91,95%CI 0.76至1.08;459名参与者,5项研究;低确定性证据)。随访4周后,使用1至3剂伊维菌素或1至3次氯菊酯治疗的完全清除率可能几乎没有差异(1至3次氯菊酯治疗的预估治愈率为93%,1至3剂伊维菌素为86%;RR 0.92,95%CI 0.82至1.03;581名参与者,5项研究;低确定性证据)。
使用标准剂量200μg/kg口服伊维菌素或1次应用5%氯菊酯洗剂治疗1周后,完全清除率可能几乎没有差异(预估治愈率:氯菊酯73%,伊维菌素68%;RR 0.93,95%CI 0.74至1.17;120名参与者,1项研究;中度确定性证据)。治疗2周后,1剂全身性伊维菌素与1次应用氯菊酯洗剂相比,可能导致相似的完全清除率(预估治愈率:两组均为67%;RR 1.00,95%CI 0.78至1.29;120名参与者,1项研究;低确定性证据)。
治疗开始4周后,标准剂量全身性伊维菌素与1%外用伊维菌素洗剂的完全清除率可能几乎没有差异(预估治愈率:口服伊维菌素97%,伊维菌素洗剂96%;RR 0.99,95%CI 0.95至1.03;272名参与者,2项研究;中度确定性证据)。同样地,4周后,与氯菊酯乳膏相比,伊维菌素洗剂的完全清除率可能几乎没有差异(预估治愈率:氯菊酯乳膏94%,伊维菌素洗剂96%;RR 1.02,95%CI 0.96至1.08;210名参与者,1项研究;中度确定性证据),不同剂量全身性伊维菌素之间也几乎没有差异(预估治愈率:2剂90%;1剂87%;RR 0.97,95%CI 0.83至1.14;80名参与者,1项研究;高确定性证据)。
纳入研究中不良事件的报告情况欠佳。全身性伊维菌素组和氯菊酯组均未因不良事件而退出研究(中度确定性证据)。治疗开始2周后,接受全身性伊维菌素或氯菊酯乳膏治疗且至少发生1起不良事件的参与者比例可能几乎没有差异(55名参与者,1项研究;中度确定性证据)。4周后,伊维菌素可能导致至少发生1起不良事件的参与者比例略高(预估发生率:氯菊酯4%,伊维菌素5%;RR 1.30,95%CI 0.35至
4.83;502名参与者,4项研究;低确定性证据)。外用伊维菌素治疗的参与者不良事件罕见且程度较轻,与全身性伊维菌素治疗相当。对于此比较,至少发生1起不良事件的参与者数量是否存在差异尚不确定(极低确定性证据)。未发生因不良事件而退出研究的情况(62名参与者,1项研究;中度确定性证据)。外用伊维菌素或氯菊酯在至少发生1起不良事件的参与者数量上是否存在差异尚不确定(极低确定性证据)。我们未发现比较不同剂量全身性伊维菌素安全性结局的研究。
我们发现,在很大程度上,氯菊酯与全身性或外用伊维菌素的疗效并无差异。总体而言,报告的不良事件较少且程度较轻。我们对效应估计值的信心大多为低到中度。报告质量差是一个主要限制因素。