Noel-Morgan Jessica, Muir William W
Center for Cardiovascular & Pulmonary Research, The Research Institute at Nationwide Children's Hospital, Columbus, OH, United States.
QTest Labs, Columbus, OH, United States.
Front Vet Sci. 2018 Mar 16;5:53. doi: 10.3389/fvets.2018.00053. eCollection 2018.
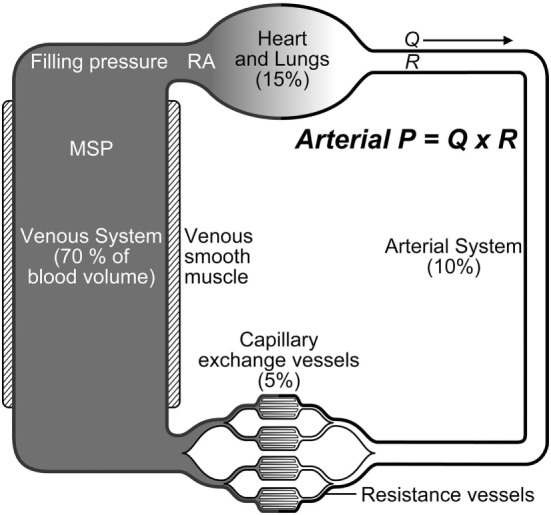
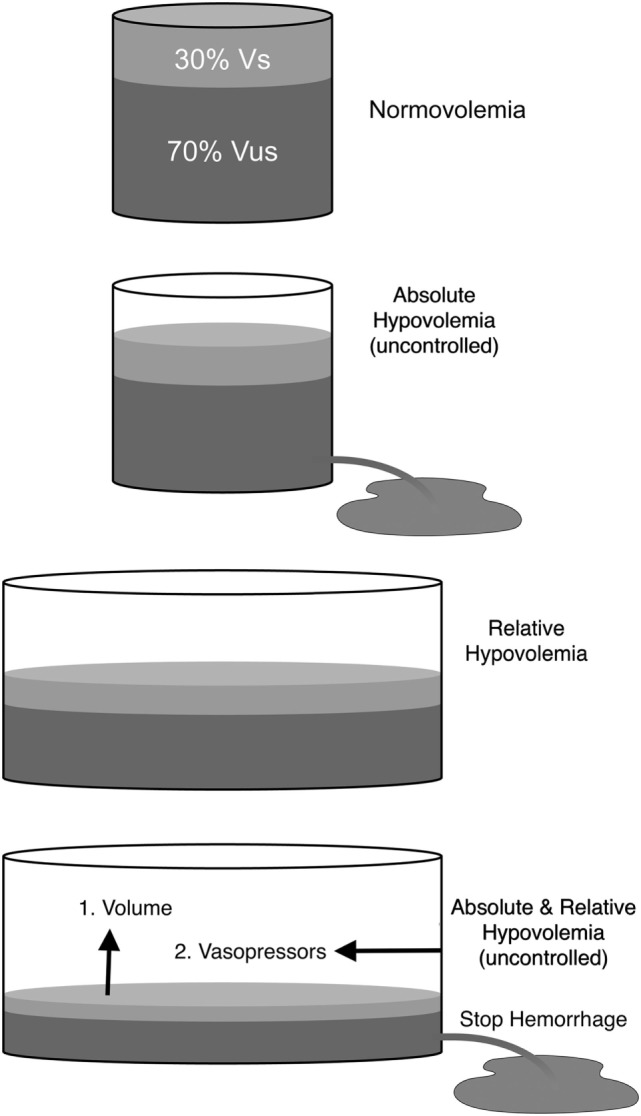
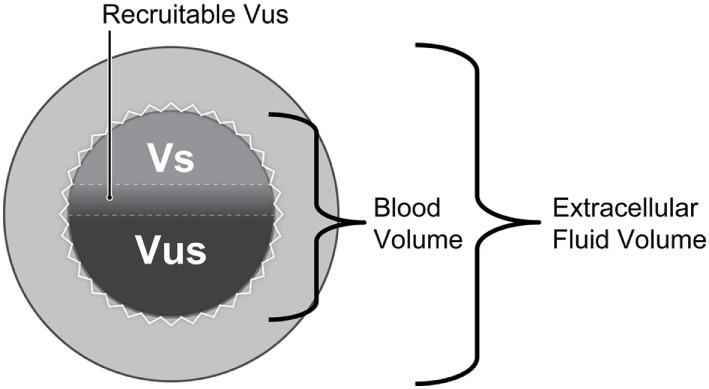
Although the utility and benefits of anesthesia and analgesia are irrefutable, their practice is not void of risks. Almost all drugs that produce anesthesia endanger cardiovascular stability by producing dose-dependent impairment of cardiac function, vascular reactivity, and compensatory autoregulatory responses. Whereas anesthesia-related depression of cardiac performance and arterial vasodilation are well recognized adverse effects contributing to anesthetic risk, far less emphasis has been placed on effects impacting venous physiology and venous return. The venous circulation, containing about 65-70% of the total blood volume, is a pivotal contributor to stroke volume and cardiac output. Vasodilation, particularly venodilation, is the primary cause of relative hypovolemia produced by anesthetic drugs and is often associated with increased venous compliance, decreased venous return, and reduced response to vasoactive substances. Depending on factors such as patient status and monitoring, a state of relative hypovolemia may remain clinically undetected, with impending consequences owing to impaired oxygen delivery and tissue perfusion. Concurrent processes related to comorbidities, hypothermia, inflammation, trauma, sepsis, or other causes of hemodynamic or metabolic compromise, may further exacerbate the condition. Despite scientific and technological advances, clinical monitoring and treatment of relative hypovolemia still pose relevant challenges to the anesthesiologist. This short perspective seeks to define relative hypovolemia, describe the venous system's role in supporting normal cardiovascular function, characterize effects of anesthetic drugs on venous physiology, and address current considerations and challenges for monitoring and treatment of relative hypovolemia, with focus on insights for future therapies.
尽管麻醉和镇痛的效用及益处无可辩驳,但其实施并非毫无风险。几乎所有产生麻醉作用的药物都会通过对心脏功能、血管反应性和代偿性自动调节反应产生剂量依赖性损害,从而危及心血管稳定性。虽然麻醉相关的心脏功能抑制和动脉血管舒张是导致麻醉风险的公认不良反应,但对影响静脉生理和静脉回流的作用却鲜有重视。静脉循环容纳了约65% - 70%的总血容量,是心输出量和每搏输出量的关键贡献因素。血管舒张,尤其是静脉舒张,是麻醉药物导致相对血容量不足的主要原因,常伴有静脉顺应性增加、静脉回流减少以及对血管活性物质反应降低。根据患者状态和监测等因素,相对血容量不足的状态在临床上可能未被察觉,由于氧输送和组织灌注受损而产生潜在后果。与合并症、体温过低、炎症、创伤、脓毒症或其他血流动力学或代谢紊乱原因相关的并发过程,可能会使病情进一步恶化。尽管有科学技术的进步,但相对血容量不足的临床监测和治疗对麻醉医生来说仍然是相关挑战。这篇简短的观点文章旨在定义相对血容量不足,描述静脉系统在支持正常心血管功能中的作用,阐述麻醉药物对静脉生理的影响,并探讨当前相对血容量不足监测和治疗的考量及挑战,重点关注未来治疗的见解。