Department of Nephrology and Medical Intensive Care, Charité - Universitätsmedizin Berlin, Berlin, Germany.
Kidney Research Institute, Division of Nephrology, University of Washington, Seattle, Washington, USA.
Kidney Int. 2018 Jun;93(6):1281-1292. doi: 10.1016/j.kint.2018.02.006. Epub 2018 Apr 12.
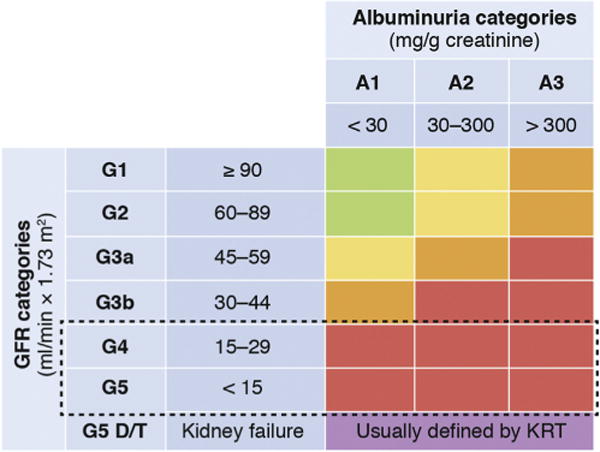
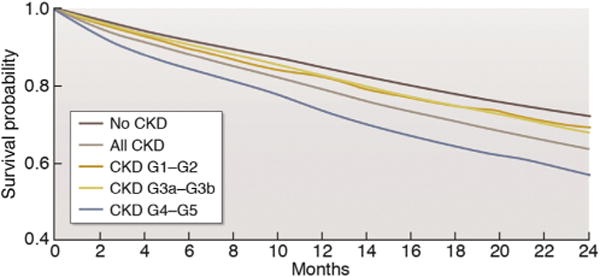
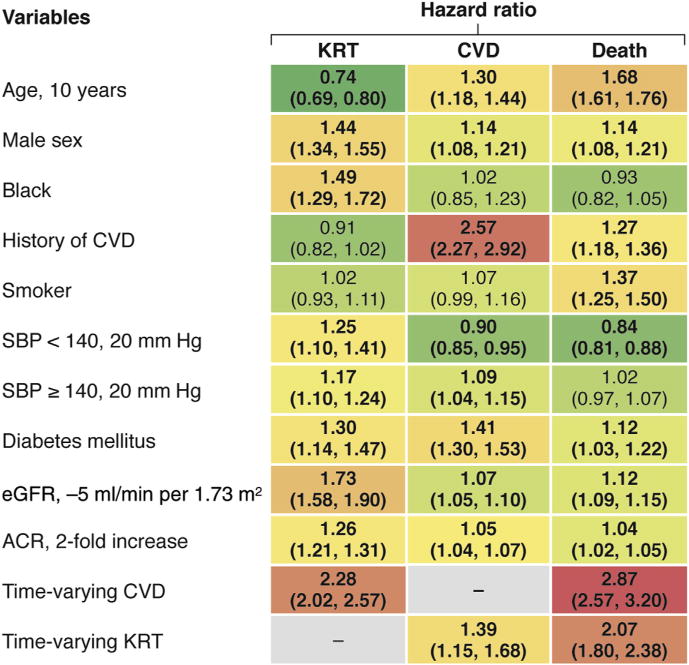
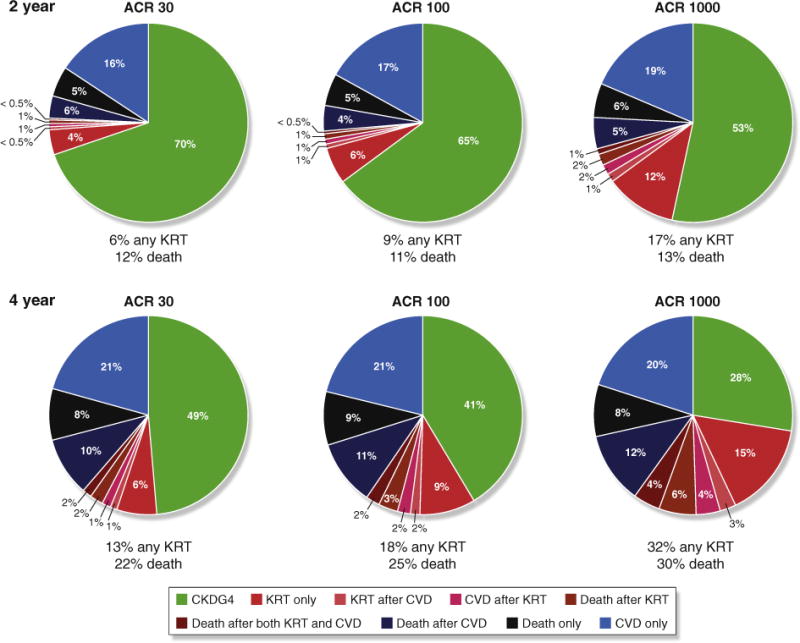
Patients with severely decreased glomerular filtration rate (GFR) (i.e., chronic kidney disease [CKD] G4+) are at increased risk for kidney failure, cardiovascular disease (CVD) events (including heart failure), and death. However, little is known about the variability of outcomes and optimal therapeutic strategies, including initiation of kidney replacement therapy (KRT). Kidney Disease: Improving Global Outcomes (KDIGO) organized a Controversies Conference with an international expert group in December 2016 to address this gap in knowledge. In collaboration with the CKD Prognosis Consortium (CKD-PC) a global meta-analysis of cohort studies (n = 264,515 individuals with CKD G4+) was conducted to better understand the timing of clinical outcomes in patients with CKD G4+ and risk factors for different outcomes. The results confirmed the prognostic value of traditional CVD risk factors in individuals with severely decreased GFR, although the risk estimates vary for kidney and CVD outcomes. A 2- and 4-year model of the probability and timing of kidney failure requiring KRT was also developed. The implications of these findings for patient management were discussed in the context of published evidence under 4 key themes: management of CKD G4+, diagnostic and therapeutic challenges of heart failure, shared decision-making, and optimization of clinical trials in CKD G4+ patients. Participants concluded that variable prognosis of patients with advanced CKD mandates individualized, risk-based management, factoring in competing risks and patient preferences.
患有严重肾小球滤过率(GFR)降低(即慢性肾脏病[CKD] G4+)的患者发生肾衰竭、心血管疾病(CVD)事件(包括心力衰竭)和死亡的风险增加。然而,对于结局的可变性和最佳治疗策略(包括开始肾脏替代治疗[KRT])知之甚少。肾脏疾病:改善全球预后(KDIGO)于 2016 年 12 月组织了一次国际专家小组的争议会议,以解决这一知识空白。与慢性肾脏病预后协作组(CKD-PC)合作,对队列研究进行了全球荟萃分析(n=264,515 名 CKD G4+患者),以更好地了解 CKD G4+患者临床结局的时机以及不同结局的危险因素。结果证实了传统 CVD 危险因素在严重 GFR 降低患者中的预后价值,尽管肾脏和 CVD 结局的风险估计值不同。还开发了一个 2 年和 4 年的 KRT 所需肾衰竭概率和时机模型。根据 4 个关键主题下的现有证据,讨论了这些发现对患者管理的影响:CKD G4+的管理、心力衰竭的诊断和治疗挑战、共同决策以及 CKD G4+患者临床试验的优化。与会者得出结论,晚期 CKD 患者的预后存在差异,需要个体化、基于风险的管理,考虑到竞争风险和患者偏好。