Houston Methodist Hospital Institute, Houston, Texas, United States of America.
Department of Biostatistics, Boston University School of Public Health, Boston, Massachusetts, United States of America.
PLoS One. 2018 Apr 16;13(4):e0196022. doi: 10.1371/journal.pone.0196022. eCollection 2018.
Estimating mortality risk during TB treatment in HIV co-infected patients is challenging for health professionals, especially in a low TB prevalence population, due to the lack of a standardized prognostic system. The current study aimed to develop and validate a simple mortality prognostic scoring system for TB/HIV co-infected patients.
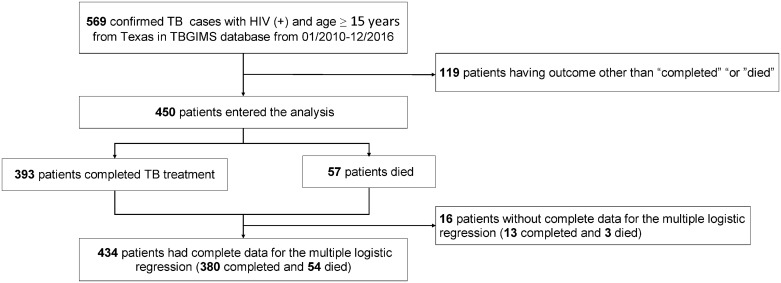
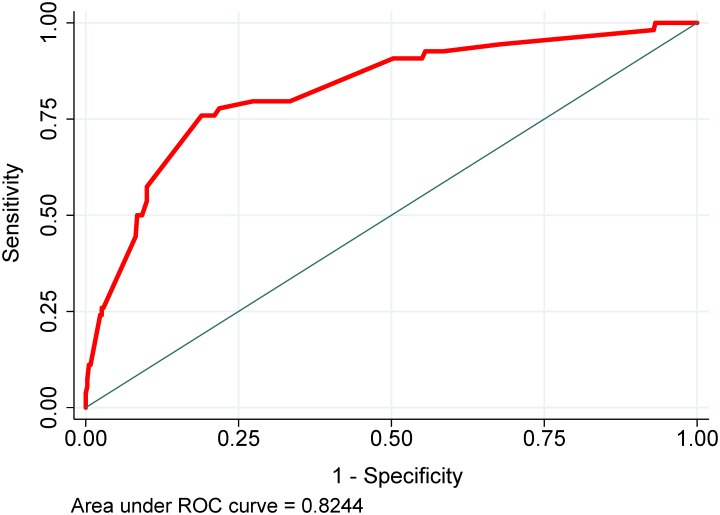
Using data from the CDC's Tuberculosis Genotyping Information Management System of TB patients in Texas reported from 01/2010 through 12/2016, age ≥15 years, HIV(+), and outcome being "completed" or "died", we developed and internally validated a mortality prognostic score using multiple logistic regression. Model discrimination was determined by the area under the receiver operating characteristic (ROC) curve (AUC). The model's good calibration was determined by a non-significant Hosmer-Lemeshow's goodness of fit test.
Among the 450 patients included in the analysis, 57 (12.7%) died during TB treatment. The final prognostic score used six characteristics (age, residence in long-term care facility, meningeal TB, chest x-ray, culture positive, and culture not converted/unknown), which are routinely collected by TB programs. Prognostic scores were categorized into three groups that predicted mortality: low-risk (<20 points), medium-risk (20-25 points) and high-risk (>25 points). The model had good discrimination and calibration (AUC = 0.82; 0.80 in bootstrap validation), and a non-significant Hosmer-Lemeshow test p = 0.71.
Our simple validated mortality prognostic scoring system can be a practical tool for health professionals in identifying TB/HIV co-infected patients with high mortality risk.
在 HIV 合并结核病患者的治疗期间,估计死亡率对卫生专业人员来说是一项挑战,尤其是在结核病低流行人群中,因为缺乏标准化的预后系统。本研究旨在为结核分枝杆菌/人类免疫缺陷病毒(HIV)合并感染患者开发和验证一种简单的死亡率预后评分系统。
利用 2010 年 1 月至 2016 年 12 月期间德克萨斯州疾病预防控制中心结核病基因分型信息管理系统中报告的年龄≥15 岁、HIV(+)、结局为“完成”或“死亡”的结核病患者的数据,我们使用多因素逻辑回归建立并内部验证了一种死亡率预后评分。通过接收者操作特征(ROC)曲线下面积(AUC)来确定模型的判别能力。通过显著的 Hosmer-Lemeshow 拟合优度检验来确定模型的良好校准。
在纳入分析的 450 例患者中,有 57 例(12.7%)在结核病治疗期间死亡。最终的预后评分使用了六个特征(年龄、长期护理机构居住、脑膜结核、胸部 X 线、培养阳性和培养未转换/未知),这些特征是结核病规划常规收集的。预后评分分为三组,预测死亡率:低危(<20 分)、中危(20-25 分)和高危(>25 分)。该模型具有良好的判别能力和校准(AUC=0.82;在 bootstrap 验证中为 0.80),且 Hosmer-Lemeshow 检验 p 值为 0.71,无统计学意义。
我们的简单验证后的死亡率预后评分系统可为识别高死亡率风险的结核分枝杆菌/人类免疫缺陷病毒(HIV)合并感染患者的卫生专业人员提供实用工具。