Department of Internal Medicine, College of Medicine, Ewha Womans University, Seoul, Republic of Korea.
Tissue Injury Defense Research Center, Ewha Womans University, Seoul, Republic of Korea.
PLoS One. 2018 Apr 26;13(4):e0195709. doi: 10.1371/journal.pone.0195709. eCollection 2018.
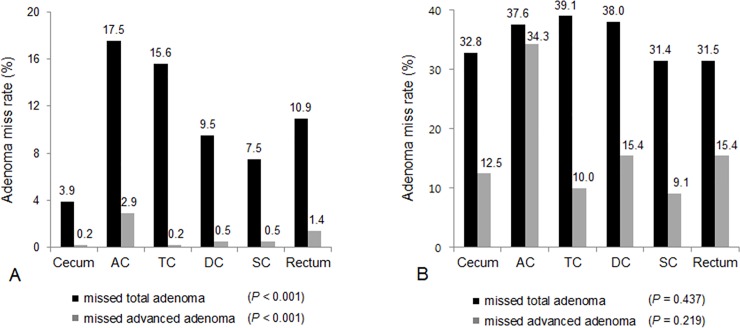
Suboptimal bowel preparation can result in missed colorectal adenoma that can evolve into interval colorectal cancer. This study aims to identify the predictive factors associated with missed adenoma on repeat colonoscopy in patients with suboptimal bowel preparation at initial colonoscopy. A total of 441 patients with suboptimal bowel preparation on initial colonoscopy and who had repeat colonoscopy within two years were included from 2007 to 2014 in six tertiary hospitals. Suboptimal bowel preparation was defined as 'poor' according to the Aronchick scale or a score ≤ 1 in at least one segment or total score < 6 according to the Boston bowel preparation scale. Of 441 patients, mean age at initial colonoscopy was 59.1 years, and 69.2% patients were male. The mean interval from initial to repeat colonoscopy was 14.1 months. The per-patient adenoma miss rate (AMR) was 42.4% for any adenoma and 5.4% for advanced adenoma. When the association between baseline clinical characteristics and missed lesions on repeat colonoscopy was analyzed, dyslipidemia (odds ratio [OR], 5.19; 95% confidence interval [CI], 1.14-23.66; P = 0.034), and high-risk adenoma (OR, 4.45; 95% CI, 1.12-17.68; P = 0.034) on initial colonoscopy were independent risk factors for missed advanced adenoma. In patients with suboptimal bowel preparation, dyslipidemia and high-risk adenoma on initial colonoscopy were independently predictive of missed advanced adenoma on repeat colonoscopy.
肠道准备不充分可能导致结直肠腺瘤漏诊,而这些腺瘤可能进展为间期结直肠癌。本研究旨在确定在初始结肠镜检查肠道准备不充分的患者中,与再次结肠镜检查时腺瘤漏诊相关的预测因素。
2007 年至 2014 年,在六家三级医院共纳入 441 例初始结肠镜检查肠道准备不充分且在两年内进行了重复结肠镜检查的患者。根据 Aronchick 量表,肠道准备不充分定义为“差”,或至少一个节段的评分≤1 分,或波士顿肠道准备量表总评分<6 分。在 441 例患者中,初始结肠镜检查时的平均年龄为 59.1 岁,69.2%为男性。从初始结肠镜检查到重复结肠镜检查的平均间隔为 14.1 个月。每位患者的腺瘤漏诊率(AMR)为任何腺瘤的 42.4%,高级别腺瘤的 5.4%。
当分析基线临床特征与重复结肠镜检查时漏诊病变之间的关系时,初始结肠镜检查时的血脂异常(比值比[OR],5.19;95%置信区间[CI],1.14-23.66;P=0.034)和高危腺瘤(OR,4.45;95%CI,1.12-17.68;P=0.034)是高级别腺瘤漏诊的独立危险因素。在肠道准备不充分的患者中,初始结肠镜检查时的血脂异常和高危腺瘤是重复结肠镜检查时高级别腺瘤漏诊的独立预测因素。