Moon Jae Hoon, Kim Ji Hoon, Lee Eun Kyung, Lee Kyu Eun, Kong Sung Hye, Kim Yeo Koon, Jung Woo Jin, Lee Chang Yoon, Yoo Roh Eul, Hwangbo Yul, Song Young Shin, Kim Min Joo, Cho Sun Wook, Kim Su Jin, Jung Eun Jae, Choi June Young, Ryu Chang Hwan, Lee You Jin, Hah Jeong Hun, Jung Yuh Seog, Ryu Junsun, Hwang Yunji, Park Sue K, Sung Ho Kyung, Yi Ka Hee, Park Do Joon, Park Young Joo
Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
Department of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
Endocrinol Metab (Seoul). 2018 Jun;33(2):278-286. doi: 10.3803/EnM.2018.33.2.278.
The ongoing Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma (MAeSTro) aims to observe the natural course of papillary thyroid microcarcinoma (PTMC), develop a protocol for active surveillance (AS), and compare the long-term prognosis, quality of life, and medical costs between the AS and immediate surgery groups.
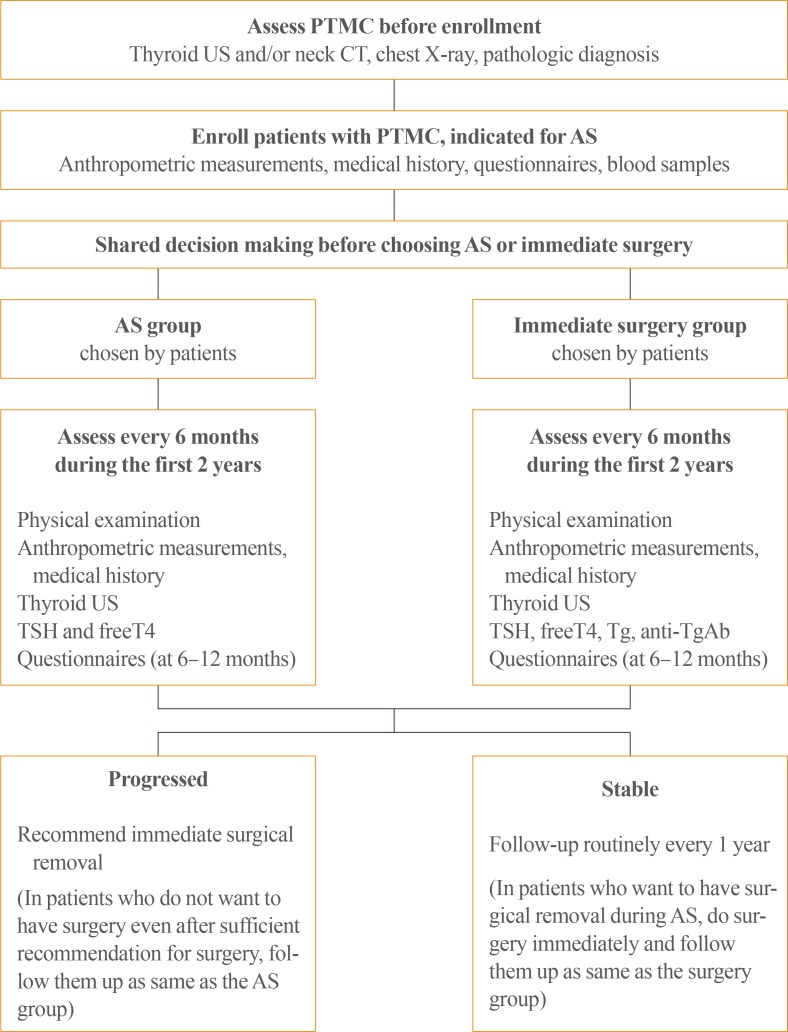
This multicenter prospective cohort study of PTMC started in June 2016. The inclusion criteria were suspicious of malignancy or malignancy based on fine needle aspiration or core needle biopsy, age of ≥18 years, and a maximum diameter of ≤1 cm. If there was no major organ involvement, no lymph node/distant metastasis, and no variants with poor prognosis, the patients were explained of the pros and cons of immediate surgery and AS before selecting AS or immediate surgery. Follow-up visits (physical examination, ultrasonography, thyroid function, and questionnaires) are scheduled every 6 months during the first 2 years, and then every 1 year thereafter. Progression was defined as a maximum diameter increase of ≥3, ≥2 mm in two dimensions, suspected organ involvement, or lymph node/distant metastasis.
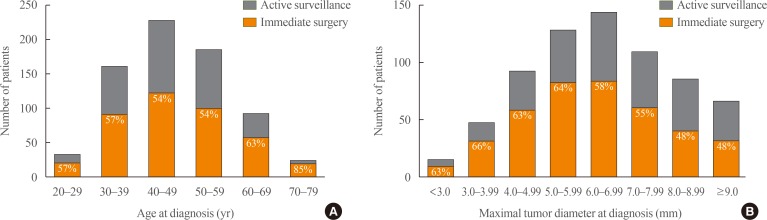
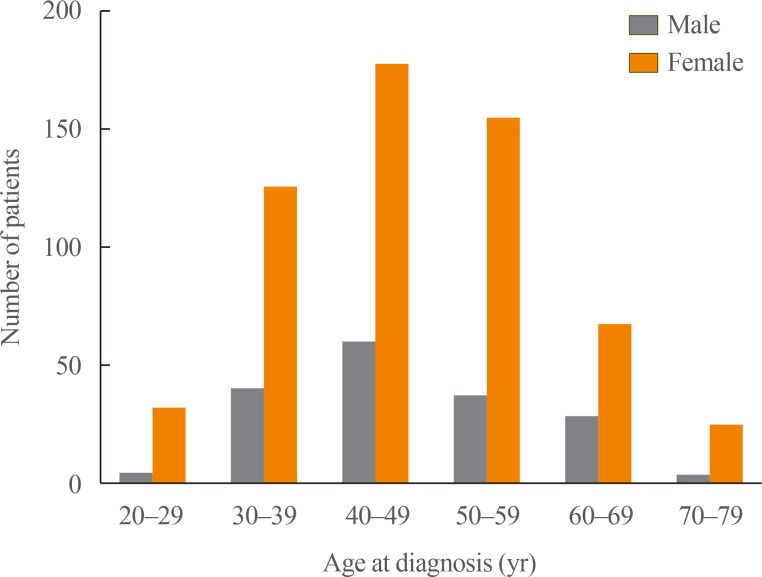
Among 439 enrolled patients, 290 patients (66.1%) chose AS and 149 patients (33.9%) chose immediate surgery. The median follow-up was 6.7 months (range, 0.2 to 11.9). The immediate surgery group had a larger maximum tumor diameter, compared to the AS group (7.1±1.9 mm vs. 6.6±2.0 mm, respectively; P=0.014).
The results will be useful for developing an appropriate PTMC treatment policy based on its natural course and risk factors for progression.
正在进行的甲状腺微小乳头状癌主动监测多中心前瞻性队列研究(MAeSTro)旨在观察甲状腺微小乳头状癌(PTMC)的自然病程,制定主动监测(AS)方案,并比较AS组和即刻手术组的长期预后、生活质量和医疗费用。
这项PTMC多中心前瞻性队列研究于2016年6月开始。纳入标准为基于细针穿刺或粗针活检怀疑为恶性或确诊为恶性、年龄≥18岁且最大直径≤1 cm。如果没有主要器官受累、没有淋巴结/远处转移且没有预后不良的变异型,在患者选择AS或即刻手术之前,向其解释即刻手术和AS的利弊。在最初2年内每6个月安排一次随访(体格检查、超声检查、甲状腺功能检查和问卷调查),此后每年一次。进展定义为最大直径在两个维度上增加≥3、≥2 mm,怀疑有器官受累,或有淋巴结/远处转移。
在439例入组患者中,290例患者(66.1%)选择了AS,149例患者(33.9%)选择了即刻手术。中位随访时间为6.7个月(范围0.2至11.9个月)。与AS组相比,即刻手术组的最大肿瘤直径更大(分别为7.1±1.9 mm和6.6±2.0 mm;P = 0.014)。
这些结果将有助于根据PTMC的自然病程和进展危险因素制定合适的治疗策略。