School of Public Health, Hawassa University, Hawassa, Ethiopia.
PLoS One. 2018 Aug 6;13(8):e0201990. doi: 10.1371/journal.pone.0201990. eCollection 2018.
In developing countries lacking functional vital registration system, statistical models are being increasingly used for estimating maternal mortality ratio (MMR). Yet, most of the models have limited applicability at sub-country level. This paper introduces a new model for estimating MMR at national and sub-national levels based on maternal health-related indicators. Further, it applies the model for explaining sub-national variations of MMR in Ethiopia.
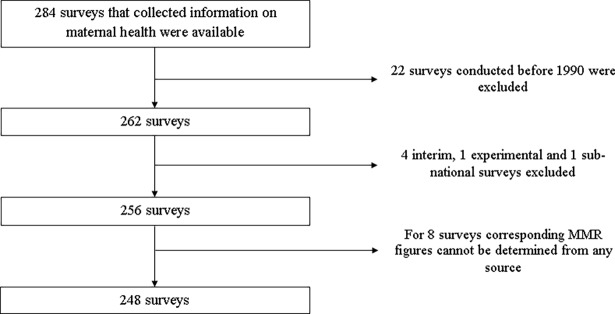
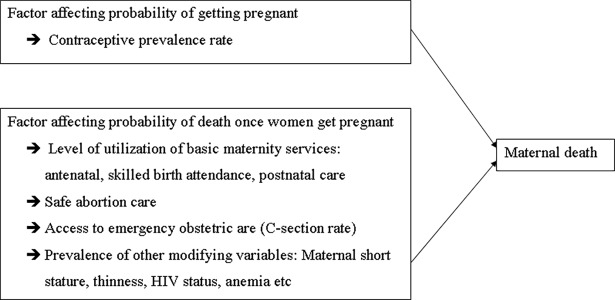
Country level data on MMR and other nine potential predictors of maternal death were extracted from 248 national Demographic and Health Surveys and other related surveys conducted in 80 low- and middle-income countries since 1990. Additional data were obtained from the World Bank and the World Health Organization databases. The potential model predictors were: contraceptive prevalence rate (CPR); utilizations of antenatal care (ANC), health institution delivery (HID), Caesarian section (CS) and postnatal care (PNC); and prevalence of maternal anemia, thinness (Body Mass Index (BMI < 18.5 kg/m2), short stature (height less than 145 cms) and HIV. Stepwise Generalized Estimating Equation (GEE) with Negative Log-binomial link was employed to model MMR as a function of the covariates.
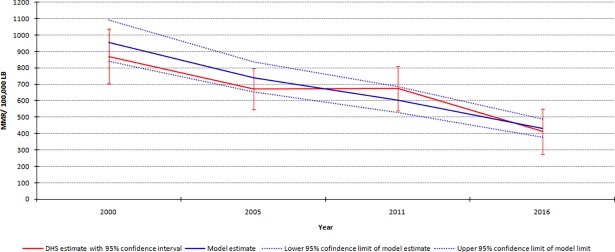
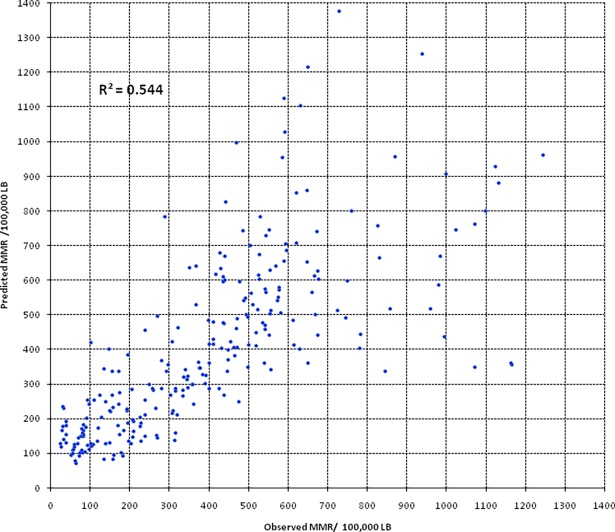
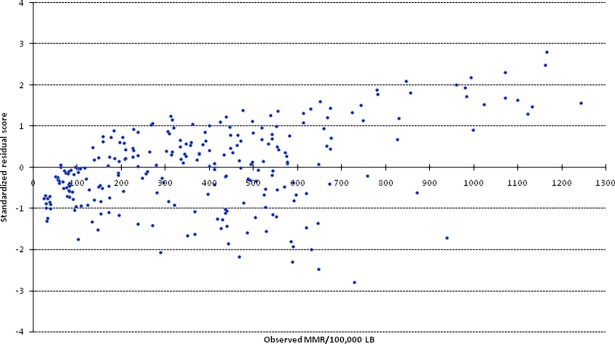
The ultimate model comprised six significant predictors and the equation is provided as: Ln (MMR) = 6.464-0.013(CPR)- 0.006(HID)- 0.003(PNC)- 0.027(CS rate) + 0.060(HIV prevalence) + 0.011 (thinness prevalence). The variation explained by the model was 54.3%) and the mean (±SD) relative standard error (8.6±2.6%) suggested the model has a reasonable precision. Application of the model to describe sub-national variation of maternal mortality in Ethiopia indicated, in 2016 the highest MMRs per 100,000 live births were in Somali (805) and Afar (795) regions. Between 2000 and 2016, all the regions of Ethiopia have significantly reduced MMRs; yet the rate of decline was lower in the aforementioned two regions. Oromiya region contributed for 46% of all maternal deaths in Ethiopia.
In developing countries lacking dependable maternal mortality data; the model can be used to estimate national and sub-national MMR with reasonable accuracy and precision.
在缺乏功能完善的生命登记系统的发展中国家,统计模型越来越多地被用于估计孕产妇死亡率(MMR)。然而,大多数模型在国家以下一级的适用性有限。本文介绍了一种基于孕产妇健康相关指标的国家和国家以下一级估计 MMR 的新模型。此外,还应用该模型解释了埃塞俄比亚孕产妇死亡率的国家以下一级差异。
从 1990 年以来在 80 个中低收入国家进行的 248 次国家人口与健康调查和其他相关调查中提取了孕产妇死亡率和其他 9 个孕产妇死亡潜在预测指标的国家数据。其他数据来自世界银行和世界卫生组织数据库。潜在的模型预测指标包括:避孕普及率(CPR);产前护理(ANC)、医疗机构分娩(HID)、剖宫产(CS)和产后护理(PNC)的利用率;以及孕产妇贫血、消瘦(体重指数(BMI<18.5kg/m2)、身材矮小(身高<145 厘米)和艾滋病毒的流行率。采用逐步广义估计方程(GEE)和负二项式链接对 MMR 作为协变量的函数进行建模。
最终模型包括六个显著的预测指标,方程如下:Ln(MMR)=6.464-0.013(CPR)-0.006(HID)-0.003(PNC)-0.027(CS 率)+0.060(HIV 流行率)+0.011(消瘦流行率)。模型解释的变异为 54.3%),平均(±SD)相对标准误差(8.6±2.6%)表明该模型具有合理的精度。该模型在描述埃塞俄比亚国家以下一级孕产妇死亡率差异方面的应用表明,2016 年每 10 万活产儿中孕产妇死亡率最高的是索马里(805)和阿法尔(795)地区。2000 年至 2016 年期间,埃塞俄比亚所有地区的孕产妇死亡率均显著下降;然而,上述两个地区的下降速度较慢。奥罗莫地区占埃塞俄比亚所有孕产妇死亡人数的 46%。
在缺乏可靠的孕产妇死亡率数据的发展中国家,可以使用该模型以合理的准确性和精度估计国家和国家以下一级的 MMR。