School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia.
Kersa Health and Demographic Surveillance Systems, Harar, Ethiopia.
J Glob Health. 2022 Jul 22;12:04051. doi: 10.7189/jogh.12.04051.
Despite registering tremendous improvement as part of the Millennium Development Goals, Ethiopia has still one of the highest numbers of maternal mortality. Although maternal mortality is one of the commonest indicators for comparison or measuring progress, its measurement remained a challenge. In a situation where, vital registration is not in place and only few women gave birth in facilities, alternative data sources from population-based surveys are essential to describe maternal deaths. In this paper, we reported estimates of maternal mortality and causes in a predominantly rural setting in eastern Ethiopia.
Data were used from the ongoing prospective open cohort of Kersa Health and Demographic Surveillance System (HDSS), located in eastern Ethiopia. At enrolment, detailed sociodemographic and household conditions were recorded for every member, followed by household visit every six months to identify any vital events: births, deaths, and migration. Whenever a death was reported, additional information about the deceased - age, sex, pregnancy status, and perceived cause of deaths - were collected through interview of the closest family member(s). Then, the probable cause of death was assigned using an automated verbal autopsy system (InterVA). In this paper, we included all deaths among women during pregnancy, childbirth or within 42 days of termination of pregnancy. To describe the trends, we calculated annual maternal mortality ratio (MMR) along with their 95% Confidence Interval (CI).
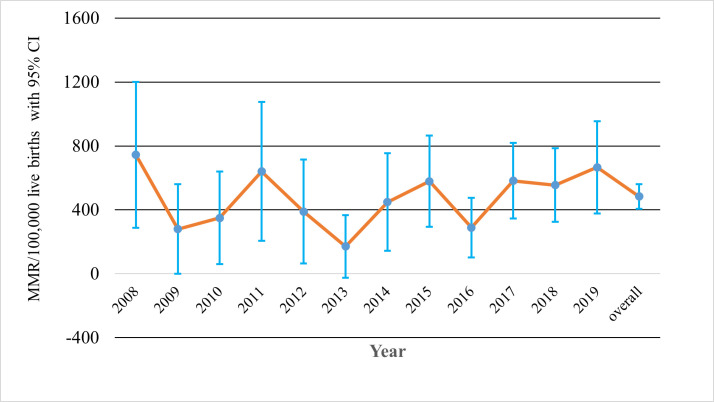
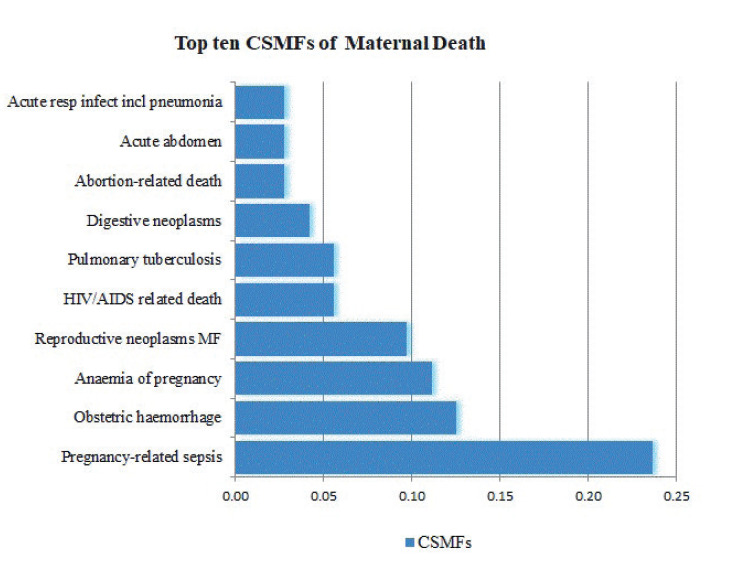
From 2008 to 2019, a total of 32 680 live births and 720 deaths among reproductive age women were registered. Of the 720 deaths, 158 (21.9%) were during pregnancy or within 42 days of termination of pregnancy, corresponding with an MMR of 484 per 100 000 live births. The three leading causes of deaths were pregnancy related sepsis, obstetric haemorrhage and anaemia of pregnancy. There was non-significant reduction in the MMR from 744 in 2008 to 665 in 2019, with three lowest ratios recorded in 2013 (172 per 100 000 live births), 2009 (280 per 100 000 live births) and 2016 (285 per 100 000 live births).
There was no significant decrement of MMR during the study period. Most deaths occurred at home from pregnancy related sepsis and haemorrhage implicating the unfinished agenda of ensuring skilled delivery and appropriate postnatal management.
尽管埃塞俄比亚作为千年发展目标的一部分取得了巨大进步,但仍是孕产妇死亡率最高的国家之一。尽管孕产妇死亡率是最常见的比较或衡量进展的指标之一,但对其进行测量仍然具有挑战性。在这种情况下,由于没有进行生命登记,只有少数妇女在设施中分娩,因此,来自人口普查的替代数据源对于描述孕产妇死亡至关重要。在本文中,我们报告了在埃塞俄比亚东部一个以农村为主的地区孕产妇死亡率和死因的估计。
数据来自位于埃塞俄比亚东部的 Kersa 卫生和人口监测系统(HDSS)正在进行的前瞻性开放式队列研究。在登记时,为每个成员记录了详细的社会人口和家庭状况,然后每六个月进行一次家访,以确定任何生命事件:出生、死亡和移民。每当报告死亡时,通过采访最亲近的家庭成员收集有关死者的更多信息 - 年龄、性别、怀孕状况和死因感知 - 然后使用自动口述尸检系统(InterVA)来分配可能的死因。在本文中,我们将怀孕期间、分娩期间或终止妊娠后 42 天内发生的所有妇女死亡都包括在内。为了描述趋势,我们计算了每年孕产妇死亡率(MMR)及其 95%置信区间(CI)。
从 2008 年到 2019 年,共登记了 32680 例活产和 720 例育龄妇女死亡。在 720 例死亡中,有 158 例(21.9%)发生在怀孕期间或终止妊娠后 42 天内,对应的孕产妇死亡率为每 100000 例活产 484 例。死亡的三个主要原因是妊娠相关败血症、产科出血和妊娠贫血。孕产妇死亡率从 2008 年的 744 人下降到 2019 年的 665 人,其中 2013 年(每 100000 例活产 172 例)、2009 年(每 100000 例活产 280 例)和 2016 年(每 100000 例活产 285 例)记录的比例最低。
在研究期间,孕产妇死亡率没有明显下降。大多数死亡发生在家中,与妊娠相关的败血症和出血有关,这表明确保熟练分娩和适当的产后管理的未完成议程。