Medical Education Unit, Gold Coast Health, Level 2 PED Building, 1 Hospital Boulevard, Southport, QLD, 4215, Australia.
School of Medicine, Griffith University, Griffith, QLD, Australia.
BMC Palliat Care. 2018 Aug 8;17(1):100. doi: 10.1186/s12904-018-0353-x.
There is a pressing need to improve end-of-life care in acute settings. This requires meeting the learning needs of all acute care healthcare professionals to develop broader clinical expertise and bring about positive change. The UK experience with the Liverpool Care of the Dying Pathway (LCP), also demonstrates a greater focus on implementation processes and daily working practices is necessary.
This qualitative study, informed by Normalisation Process Theory (NPT), investigates how a tool for end-of-life care was embedded in a large Australian teaching hospital. The study identified contextual barriers and facilitators captured in real time, as the 'Clinical Guidelines for Dying Patients' (CgDp) were implemented. A purposive sample of 28 acute ward (allied health 7 [including occupational therapist, pharmacists, physiotherapist, psychologist, speech pathologist], nursing 10, medical 8) and palliative care (medical 2, nursing 1) staff participated. Interviews (n = 18) and focus groups (n = 2), were audio-recorded and transcribed verbatim. Data were analysed using an a priori framework of NPT constructs; coherence, cognitive participation, collective action and reflexive monitoring.
The CgDp afforded staff support, but the reality of the clinical process was invariably perceived as more complex than the guidelines suggested. The CgDp 'made sense' to nursing and medical staff, but, because allied health staff were not ward-based, they were not as engaged (coherence). Implementation was challenged by competing concerns in the acute setting where most patients required a different care approach (cognitive participation). The CgDp is designed to start when a patient is dying, yet staff found it difficult to diagnose dying. Staff were concerned that they lacked ready access to experts (collective action) to support this. Participants believed using CgDp improved patient care, but there was an absence of participation in real time monitoring or quality improvement activity.
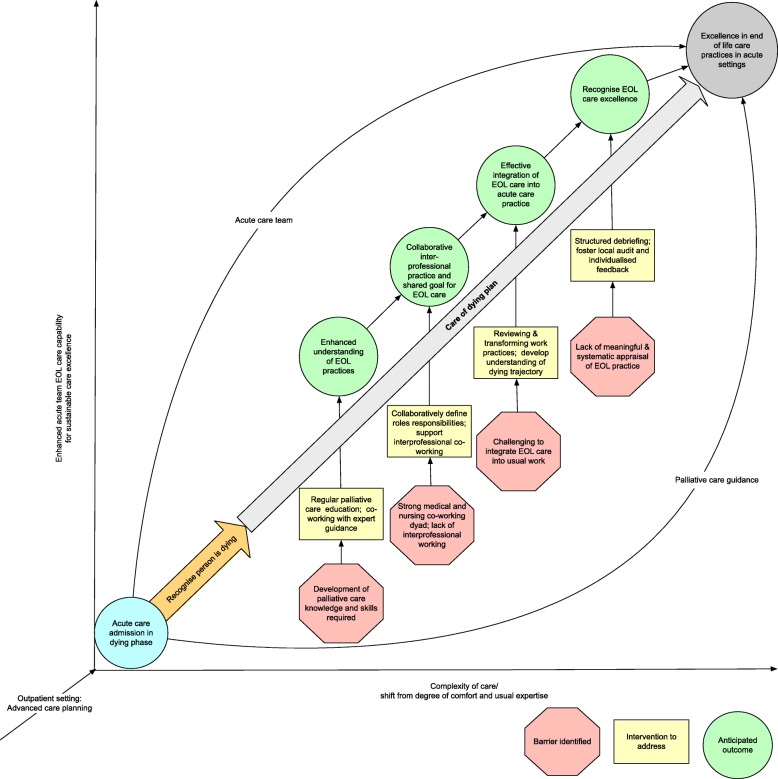
We propose a model, which addresses the risks and barriers identified, to guide implementation of end-of-life care tools in acute settings. The model promotes interprofessional and interdisciplinary working and learning strategies to develop capabilities for embedding end of life (EOL) care excellence whilst guided by experienced palliative care teams. Further research is needed to determine if this model can be prospectively applied to positively influence EOL practices.
在急症环境中,提高临终关怀质量的需求迫在眉睫。这需要满足所有急症医疗保健专业人员的学习需求,以培养更广泛的临床专业知识并带来积极的改变。英国在推行利物浦临终关怀途径(LCP)方面的经验也表明,需要更加关注实施过程和日常工作实践。
本研究采用常规进程理论(NPT),调查了一种临终关怀工具如何在澳大利亚一家大型教学医院中得到应用。该研究实时确定了实施“临终患者临床指南”(CgDp)过程中的背景障碍和促进因素。研究采用目的性抽样法,选取了 28 名急症病房(包括职业治疗师、药剂师、物理治疗师、心理学家、言语病理学家在内的联合健康科 7 名,护士 10 名,医生 8 名)和姑息治疗(医生 2 名,护士 1 名)的工作人员参与研究。共进行了 18 次访谈(n=18)和 2 次焦点小组(n=2),并对音频记录进行了逐字转录。使用 NPT 结构的预先设定框架(一致性、认知参与、集体行动和反思性监测)对数据进行了分析。
CgDp 为员工提供了支持,但临床过程的实际情况总是比指南所建议的更为复杂。CgDp 得到了护理和医务人员的认可,但由于联合健康科工作人员不在病房工作,他们的参与度较低(一致性)。在以急症为主的环境中,CgDp 的实施受到了各种竞争因素的挑战,因为大多数患者需要不同的护理方法(认知参与)。CgDp 的设计目的是在患者临终时开始使用,但工作人员发现难以确定患者是否处于临终状态。工作人员担心他们无法随时获得专家的支持(集体行动)。参与者认为使用 CgDp 可以改善患者的护理质量,但缺乏实时监测或质量改进活动的参与。
我们提出了一个模型,该模型解决了识别出的风险和障碍,以指导在急症环境中实施临终关怀工具。该模型促进了跨专业和跨学科的工作和学习策略,以发展临终关怀卓越的能力,同时由经验丰富的姑息治疗团队指导。需要进一步研究以确定该模型是否可以前瞻性地应用,以积极影响临终关怀实践。