Pawaskar Manjiri D, Xu Liou, Tang Yuexin, Puckrein Gary A, Rajpathak Swapnil N, Stuart Bruce
Merck & Co., Inc., Kenilworth, NJ, USA.
National Minority Quality Forums, Washington, DC, USA.
Diabetes Ther. 2018 Oct;9(5):1979-1993. doi: 10.1007/s13300-018-0489-y. Epub 2018 Aug 24.
Nonadherence to antihyperglycemic agents (AHAs) increases the incidence of morbidity and mortality, as well as healthcare-related costs, in patients with type 2 diabetes (T2D). This study examined the association between medication copayment and adherence and discontinuation among elderly patients with T2D who use generic versus branded AHAs.
A retrospective, observational cohort study used Medicare administrative claims data (index period: 1 June 2012 to 31 December 2013). Drug copayments were measured as the copayment of the index medication for a 30-day supply after patients met their plan deductible. Patients were stratified into a branded or generic cohort based on the index medication. Adherence was measured by the proportion of days covered (≥ 80%) and discontinuation by a treatment gap of > 60 days in 10 months during the follow-up period. Poisson regressions were conducted for medication adherence and discontinuation, while controlling for demographic, clinical, and comorbid conditions.
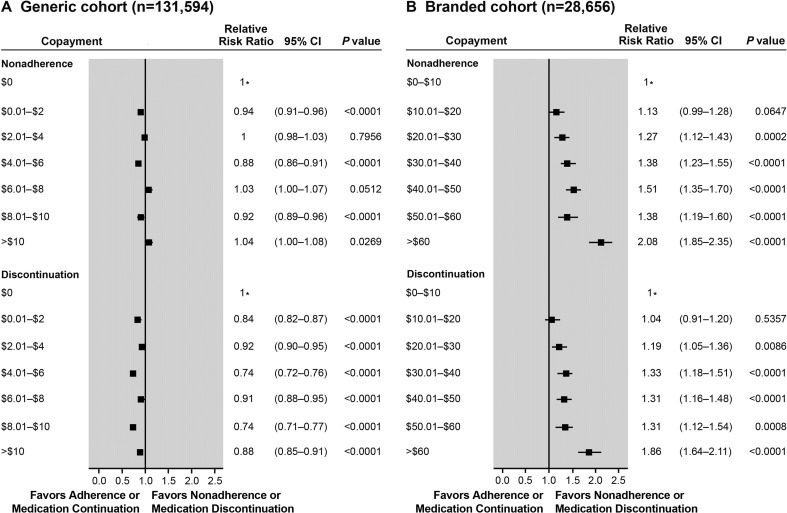
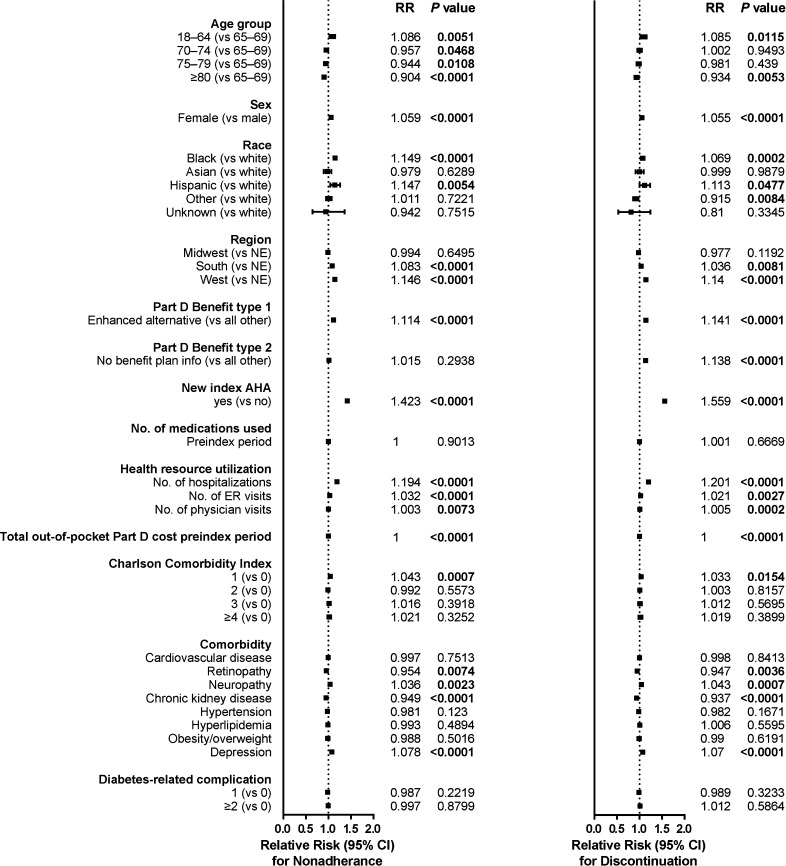
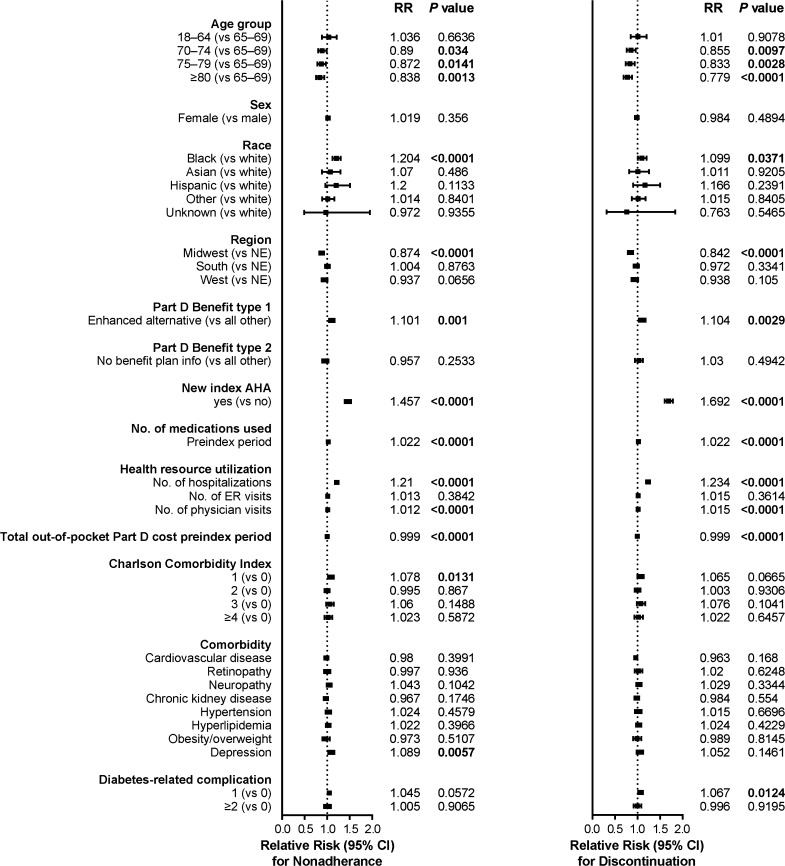
Overall, 160,250 patients on AHA monotherapy were included in the analysis; 131,594 (82%) were prescribed a generic and 28,656 (18%) a branded AHA with a mean copay of $6 and $41, respectively. Increases in copayment increased nonadherence and discontinuation for branded medications but not for generic AHA medications. In both cohorts, elderly patients (≥ 75 years of age) had a lower risk of nonadherence and discontinuation. Black patients had a higher risk of nonadherence or discontinuing medication. Patients having more frequent inpatient, emergency room, and/or physician visits were at higher risk of nonadherence or discontinuing therapy in the branded and generic cohorts (P < 0.001).
The impact of drug copayment on adherence and discontinuation varied considerably between branded and generic AHAs. Medicare patients taking branded AHAs had a higher risk of nonadherence with increasing copayment and were more likely to discontinue medication, whereas this association was not observed in patients taking generic medications.
Merck & Co, Inc., Kenilworth, NJ, USA. Plain language summary available for this article.
2型糖尿病(T2D)患者不坚持服用抗高血糖药物(AHA)会增加发病率、死亡率以及医疗相关费用。本研究探讨了使用通用型与品牌型AHA的老年T2D患者中药物自付费用与药物依从性及停药之间的关联。
一项回顾性观察队列研究使用了医疗保险行政索赔数据(索引期:2012年6月1日至2013年12月31日)。药物自付费用以患者达到计划免赔额后30天用量的索引药物自付费用来衡量。根据索引药物将患者分为品牌型或通用型队列。依从性通过覆盖天数比例(≥80%)来衡量,停药则通过随访期间10个月内治疗间隔>60天来衡量。对药物依从性和停药情况进行泊松回归分析,同时控制人口统计学、临床和合并症情况。
总体而言,160250例接受AHA单药治疗的患者纳入分析;131594例(82%)被开具通用型AHA,28656例(18%)被开具品牌型AHA,平均自付费用分别为6美元和41美元。自付费用增加会增加品牌药物的不依从性和停药率,但通用型AHA药物则不然。在两个队列中,老年患者(≥75岁)不依从和停药的风险较低。黑人患者不依从或停药的风险较高。在品牌型和通用型队列中,住院、急诊室和/或看医生更频繁的患者不依从或停药的风险更高(P<0.001)。
药物自付费用对依从性和停药的影响在品牌型和通用型AHA之间有很大差异。服用品牌型AHA的医疗保险患者随着自付费用增加不依从风险更高,更有可能停药,而服用通用型药物的患者未观察到这种关联。
美国新泽西州肯尼沃思市默克公司。本文提供通俗易懂的摘要。