Cardiovascular Clinical Research Center, Leon H. Charney Division of Cardiology, Department of Medicine, New York University School of Medicine, New York, NY, United States of America.
Department of Medicine, Montefiore Medical Center, Albert Einstein School of Medicine, Bronx, NY, United States of America.
Int J Cardiol. 2019 Jan 1;274:16-20. doi: 10.1016/j.ijcard.2018.08.103. Epub 2018 Sep 1.
Myocardial infarction (MI) presentations are more common during winter months and morning hours. However, it is unknown whether MI with obstructive coronary artery disease (MI-CAD) and non-obstructive CAD (MINOCA) display similar patterns.
We evaluated seasonal and circadian patterns of MI presentation by coronary artery disease (CAD) status and sex in patients with MI from 2007 to 2014 in the National Cardiovascular Data Registry (NCDR) Acute Coronary Treatment Intervention Outcomes Network (ACTION) Registry-Get With the Guidelines. Adult patients who underwent coronary angiography for MI were included. Patients with missing age, sex, or angiographic data, cocaine use, thrombolytic therapy prior to catheterization, or prior revascularization were excluded. Baseline demographics and characteristics of symptom onset, including season and time of day of presentation, were compared by CAD status and sex.
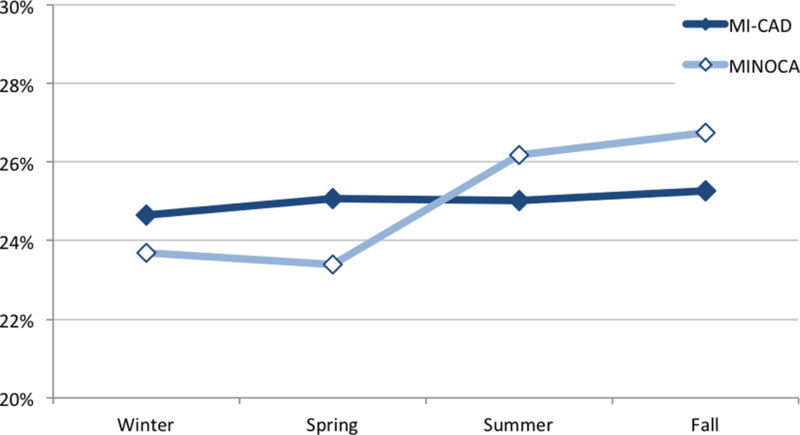
Among 322,523 patients, 112,547 were female (35%); 18,918 had MINOCA (5.9%). There was no seasonal pattern of MI overall. However, both men and women with MINOCA presented more often in the summer and fall while MI-CAD presentations were equally distributed across seasons. The most common time of presentation was 8 am-2 pm regardless of CAD status or sex. A secondary peak in women with MINOCA during late afternoon hours was also identified.
Seasonal variation of MI differed between MINOCA and MI-CAD, with a small increase in MINOCA incidence in the summer and fall. MINOCA and MI-CAD most commonly occurred in the morning, with a secondary peak in late afternoon in women with MINOCA. These differences in presentation may relate to underlying MI pathophysiology.
心肌梗死(MI)的发作在冬季和清晨更为常见。然而,尚不清楚是否伴有阻塞性冠状动脉疾病(MI-CAD)和非阻塞性 CAD(MINOCA)的 MI 具有相似的发作模式。
我们评估了 2007 年至 2014 年期间,在国家心血管数据注册(NCDR)急性冠状动脉治疗干预结果网络(ACTION)注册-GET WITH THE GUIDELINES 中,MI 患者的冠状动脉疾病(CAD)状态和性别与心肌梗死发作的季节性和昼夜节律模式。纳入接受 MI 冠状动脉造影的成年患者。排除年龄、性别或血管造影数据缺失、可卡因使用、血管成形术前溶栓治疗或既往血运重建的患者。比较 CAD 状态和性别患者的基线人口统计学特征和症状发作特征,包括发作时的季节和时间。
在 322523 例患者中,有 112547 例女性(35%),18918 例为 MINOCA(5.9%)。总体而言,MI 无季节性发作模式。然而,MINOCA 患者无论男性还是女性,在夏季和秋季的发作更为常见,而 MI-CAD 的发作则在各个季节均有分布。无论 CAD 状态或性别如何,最常见的发作时间均为上午 8 点至下午 2 点。MINOCA 女性患者还发现下午晚些时候有一个次要高峰。
MINOCA 和 MI-CAD 之间的 MI 季节性变化不同,MINOCA 的发病率在夏季和秋季略有增加。MINOCA 和 MI-CAD 最常发生在上午,MINOCA 女性在下午晚些时候出现第二个高峰。这些发作模式的差异可能与潜在的 MI 病理生理学有关。