Bielski Andrzej, Rivas Eva, Ruetzler Kurt, Smereka Jacek, Puslecki Mateusz, Dabrowski Marek, Ladny Jerzy R, Frass Michael, Robak Oliver, Evrin Togay, Szarpak Lukasz
Polish Society of Disaster Medicine.
Department of Anesthesiology, Hospital Clinic, IDIBAPS (Institut d'Investigacions Biomèdiques August Pi i Sunyer), University of Barcelona, Barcelona, Spain.
Medicine (Baltimore). 2018 Oct;97(40):e12593. doi: 10.1097/MD.0000000000012593.
Securing the airway and enabling adequate oxygenation and ventilation is essential during cardiopulmonary resuscitation (CPR). The aim of the study was to evaluate the success rate of blind intubation via the I-Gel and the Air-Q compared with direct laryngoscopy guided endotracheal intubation by inexperienced physician and to measure time to successful intubation.
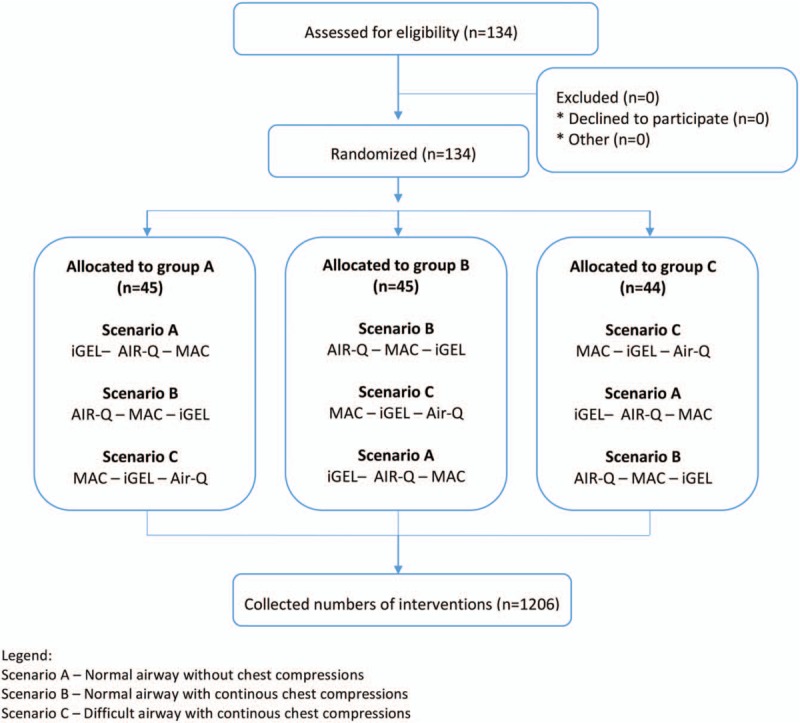
The study was designed as a randomized, cross-over simulation study. A total of 134 physicians, from specialties other than Anesthesia or Emergency Medicine, who considered themselves skilled in endotracheal intubation but who have never used any kind of supraglottic airway device performed blind intubation via the I-Gel and Air-Q and direct laryngoscopy guided endotracheal intubation in 3 randomized scenarios: normal airway without chest compression during intubation attempt; normal airway with continuous chest compression during intubation attempt; difficult airway with continuous chest compression.
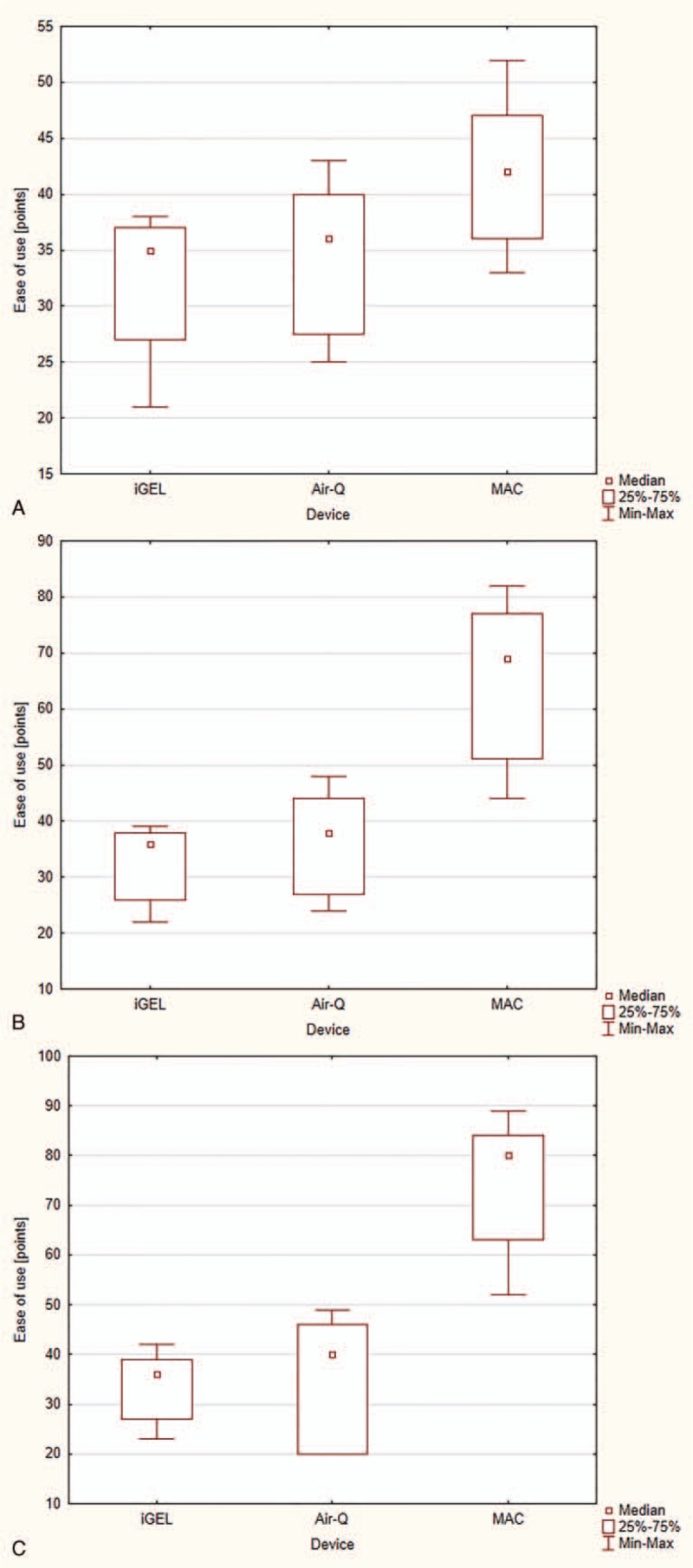
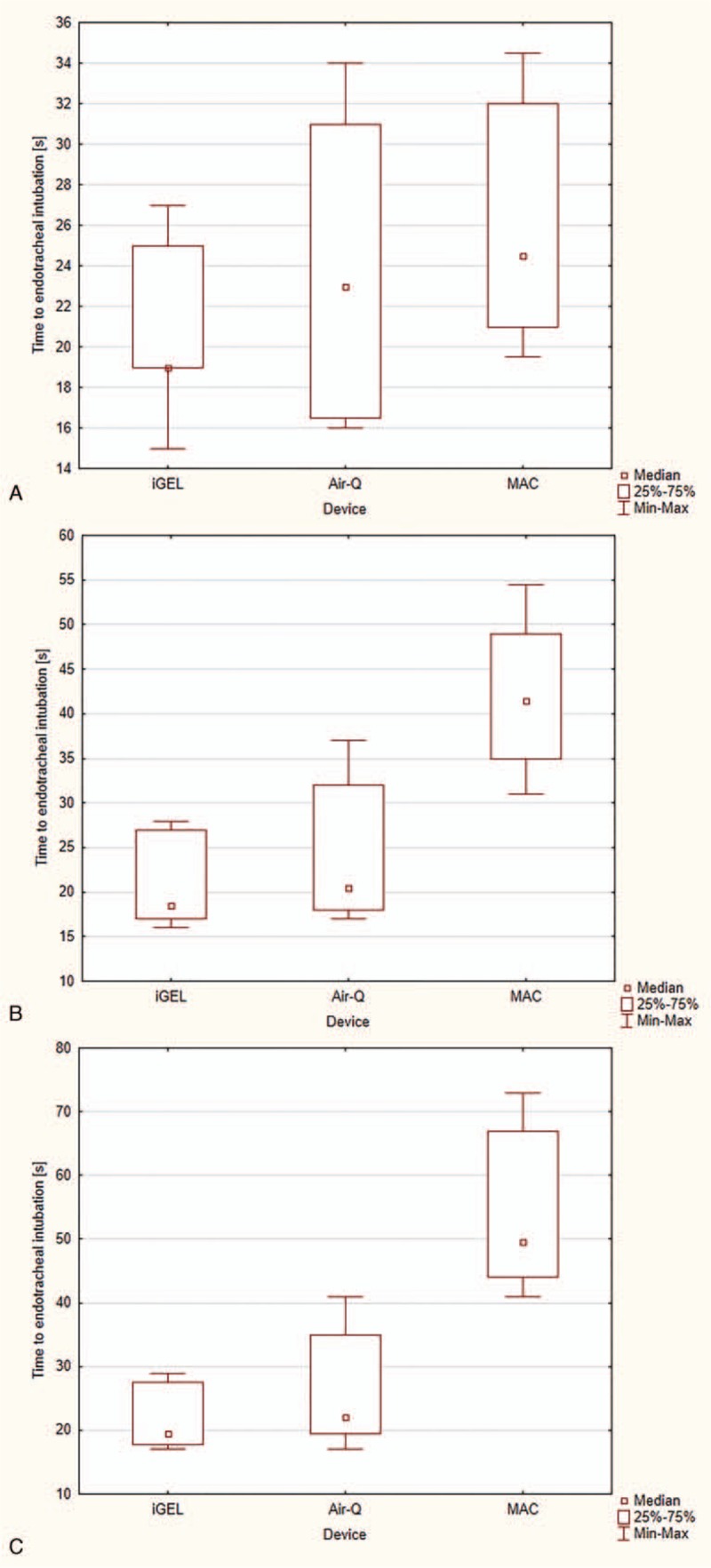
Scenario A: Success rate with initial intubation attempt was 72% for endotracheal intubation, 75% in Air-Q, and 81% in I-Gel. Time to endotracheal intubation and ease of intubation was comparable with all 3 airway devices used. Scenario B: Success rate with the initial intubation attempt was 42% for endotracheal intubation, compared with 75% in Air-Q and 80% in I-Gel. Time for endotracheal intubation was significantly prolonged in endotracheal intubation (42 seconds, 35-49), compared with Air-Q (21 seconds, 18-32) and I-Gel (19 seconds, 17-27). Scenario C: The success rate with the initial intubation attempt was 23% in endotracheal intubation, compared with 65% in Air-Q and 74% in I-Gel. Time to intubation was comparable with both supraglottic airway devices (20 vs 22 seconds) but was significantly shorter compared with endotracheal intubation (50 seconds, P < .001).
Less to moderately experienced providers are able to perform endotracheal intubation in easy airways but fail during ongoing chest compressions and simulated difficult airway. Consequently, less to moderately experienced providers should refrain from endotracheal intubation during ongoing chest compressions during CPR and in expected difficult airways. Supraglottic airway devices are reliable alternatives and blind intubation through these devices is a valuable airway management strategy.
在心肺复苏(CPR)期间确保气道安全并实现充分的氧合和通气至关重要。本研究的目的是评估与经验不足的医生进行直接喉镜引导气管插管相比,通过I-Gel和Air-Q进行盲插的成功率,并测量成功插管的时间。
本研究设计为一项随机交叉模拟研究。共有134名来自麻醉或急诊医学以外专业的医生,他们自认为擅长气管插管,但从未使用过任何类型的声门上气道装置,在3种随机场景下分别通过I-Gel和Air-Q进行盲插以及直接喉镜引导气管插管:插管尝试期间气道正常且无胸外按压;插管尝试期间气道正常且持续胸外按压;困难气道且持续胸外按压。
场景A:初次插管尝试时,气管插管的成功率为72%,Air-Q为75%,I-Gel为81%。使用所有3种气道装置时,气管插管时间和插管难易程度相当。场景B:初次插管尝试时,气管插管的成功率为42%,相比之下Air-Q为75%,I-Gel为80%。气管插管的插管时间显著延长(42秒,35 - 49),相比之下Air-Q为(21秒,18 - 32),I-Gel为(19秒,17 - 27)。场景C:初次插管尝试时,气管插管的成功率为23%,相比之下Air-Q为65%,I-Gel为74%。与两种声门上气道装置相比,插管时间相当(20秒对22秒),但与气管插管相比显著更短(50秒,P < 0.001)。
经验较少至中等的医护人员能够在简单气道中进行气管插管,但在持续胸外按压和模拟困难气道时会失败。因此,经验较少至中等的医护人员在CPR期间持续胸外按压时以及在预期的困难气道中应避免进行气管插管。声门上气道装置是可靠的替代方法,通过这些装置进行盲插是一种有价值的气道管理策略。