Chiu Michael H, Miller Robert J H, Barry Rebecca, Li Bing, Har Bryan J, Wilton Stephen B, Knudtson Merril, Howlett Jonathan G, James Matthew T
Department of Cardiac Sciences, Libin Cardiovascular Institute of Alberta, Cumming School of Medicine, University of Calgary, AB, Canada.
Libin Cardiovascular Institute of Alberta, Cumming School of Medicine, University of Calgary, AB, Canada.
Can J Kidney Health Dis. 2018 Oct 15;5:2054358118804838. doi: 10.1177/2054358118804838. eCollection 2018.
Angiotensin-converting enzyme inhibitors/angiotensin receptor blocker (ACE-I/ARB) improve outcomes in patients with heart failure and reduced left-ventricular (LV) systolic function. However, these medications can cause a rise in serum creatinine and their benefits in patients with HF accompanied by kidney disease are less certain.
To characterize associations between estimated glomerular filtration rate (eGFR), patterns of ACE-Is and ARBs use, and 1-year survival following hospitalization for heart failure (HF).
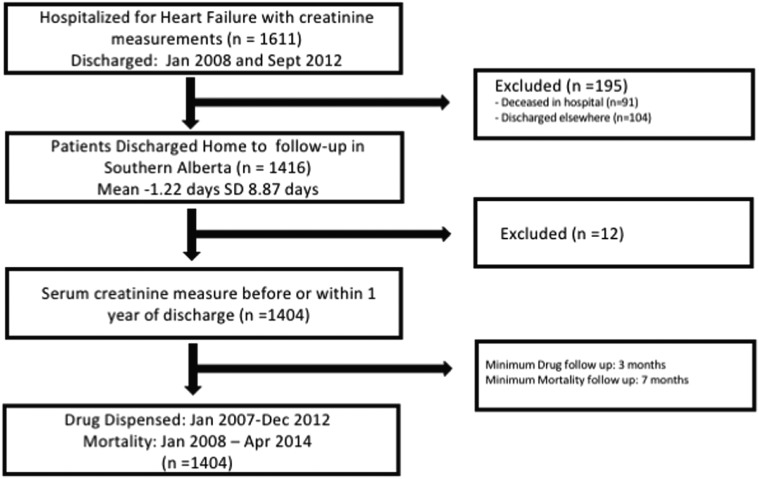
We formed a retrospective cohort study of patients admitted with HF and followed HF medication prescriptions using the pharmaceutical information network, stratified by discharge eGFR.
Cardiology services in 3 centers in Southern Alberta, Canada.
The study cohort included patients admitted to hospital with a clinical diagnosis of HF.
eGFR was determined from inpatient laboratory data prior to discharge. Outpatient prescription data prior to and following the index hospitalization was obtained using the Pharmaceutical Information Network of Alberta and survival was determined from provincial vital statistics.
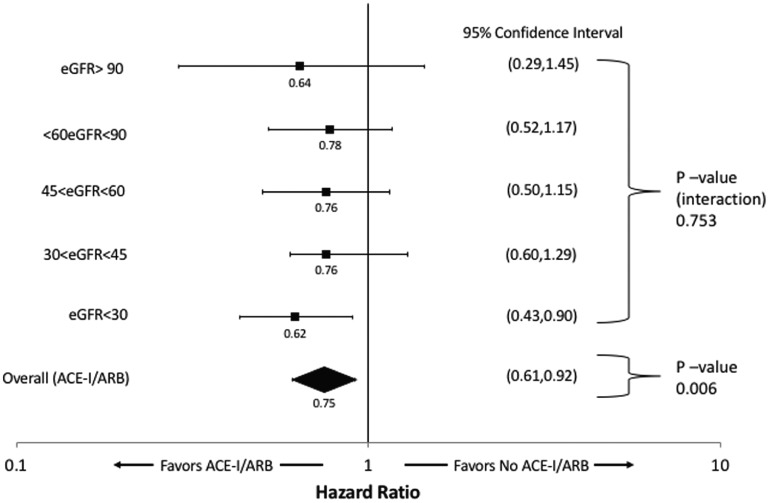
Characteristics of the HF cohort were obtained from the Admissions Module of the Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH) database. Multivariable Cox proportional hazards models were used to evaluate the association between time-varying ACE-I/ARB use, and mortality, and to test whether eGFR modified this association.
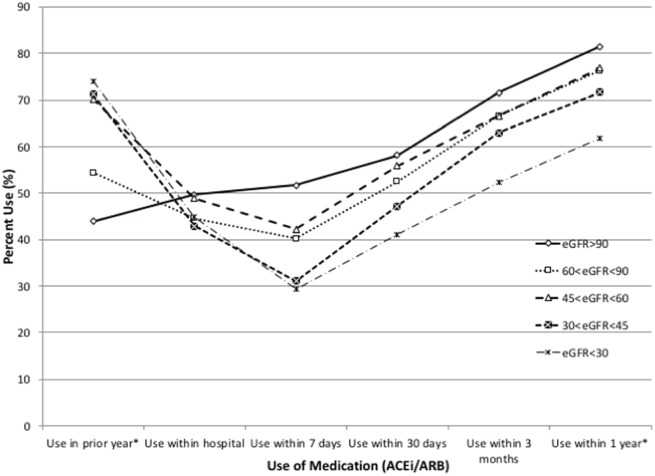
Totally, 1404 patients were included. Within the first 3 months following discharge, ACE-I/ARBs were used in 71%, 67%, 62%, and 52% for those with eGFR > 90, 45-89, 30-44, and < 30 mL/min/1.73 m, respectively, with differences in use persisting after 1 year of follow-up. Patients with eGFR < 45 mL/min/1.73 m had significantly lower rates of ACE-I/ARB use following hospitalization. In adjusted models, ACE-I/ARB use following discharge was associated with 25% lower risk of mortality (Hazard Ratio [HR]: 0.75, 95% confidence interval [CI]: 0.61-0.92; < 0.01), without evidence that this association differed by eGFR ( = 0.75).
LV function measurements were not available for the cohort. Due to the observation design of the study, treatment-selection bias may be present.
Patients with HF and reduced eGFR at time of hospital discharge were less likely to receive ACE-I/ARB despite these medications being associated with lower mortality independent of eGFR. These findings demonstrate the need for further research on strategies for safe use of ACE-I and ARB in patients with HF and kidney disease.
血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂(ACE-I/ARB)可改善心力衰竭且左心室(LV)收缩功能降低患者的预后。然而,这些药物可导致血清肌酐升高,其在伴有肾脏疾病的心力衰竭患者中的益处尚不确定。
描述估计肾小球滤过率(eGFR)、ACE-I和ARB使用模式与心力衰竭(HF)住院后1年生存率之间的关联。
我们对因HF入院的患者进行了一项回顾性队列研究,并使用药物信息网络跟踪HF药物处方,按出院时的eGFR分层。
加拿大艾伯塔省南部3个中心的心脏病科服务。
研究队列包括临床诊断为HF的住院患者。
eGFR根据出院前的住院实验室数据确定。使用艾伯塔省药物信息网络获取索引住院前后的门诊处方数据,并根据省级生命统计数据确定生存率。
HF队列的特征来自艾伯塔省冠心病结局评估项目(APPROACH)数据库的入院模块。多变量Cox比例风险模型用于评估随时间变化的ACE-I/ARB使用与死亡率之间的关联,并检验eGFR是否改变了这种关联。
总共纳入了1404例患者。出院后的前3个月内,eGFR>90、45-89、30-44和<30 mL/min/1.73 m²的患者使用ACE-I/ARB的比例分别为71%、67%、62%和52%,随访1年后使用情况仍存在差异。eGFR<45 mL/min/1.73 m²的患者住院后使用ACE-I/ARB的比例显著较低。在调整模型中,出院后使用ACE-I/ARB与死亡风险降低25%相关(风险比[HR]:0.75,95%置信区间[CI]:0.61-0.92;P<0.01),没有证据表明这种关联因eGFR而异(P=0.75)。
该队列无法获得LV功能测量值。由于研究的观察性设计,可能存在治疗选择偏倚。
出院时eGFR降低的HF患者接受ACE-I/ARB的可能性较小,尽管这些药物与较低的死亡率相关,且与eGFR无关。这些发现表明需要进一步研究在HF和肾脏疾病患者中安全使用ACE-I和ARB的策略。