a Department of Emergency , Dongfang Hospital Beijing University of Chinese Medicine , Beijing , China.
b Department of Emergency , Beijing University of Chinese Medicine Third Affiliated Hospital , Beijing , China.
Drug Deliv. 2018 Nov;25(1):1898-1909. doi: 10.1080/10717544.2018.1523257.
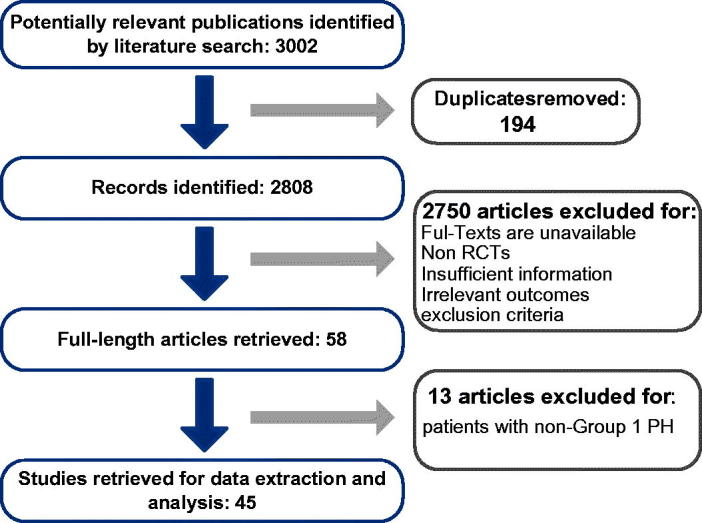
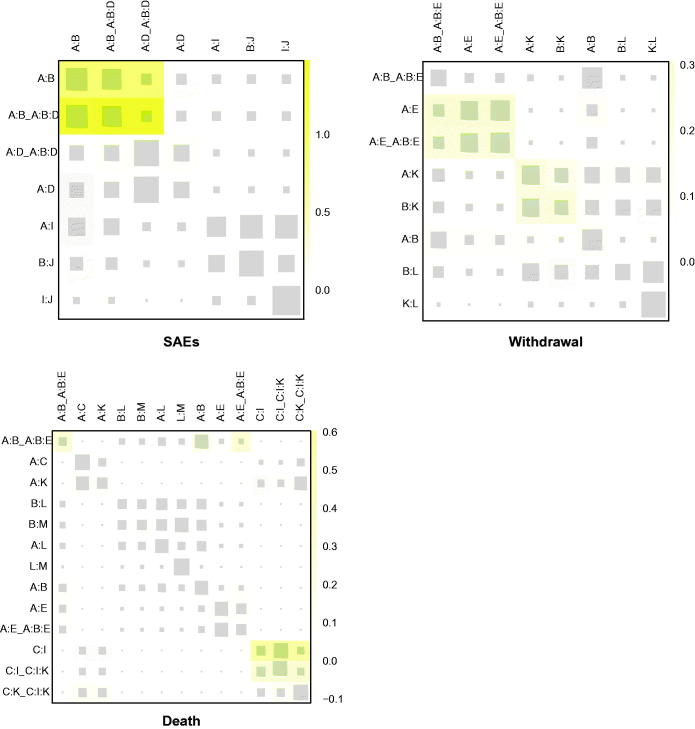
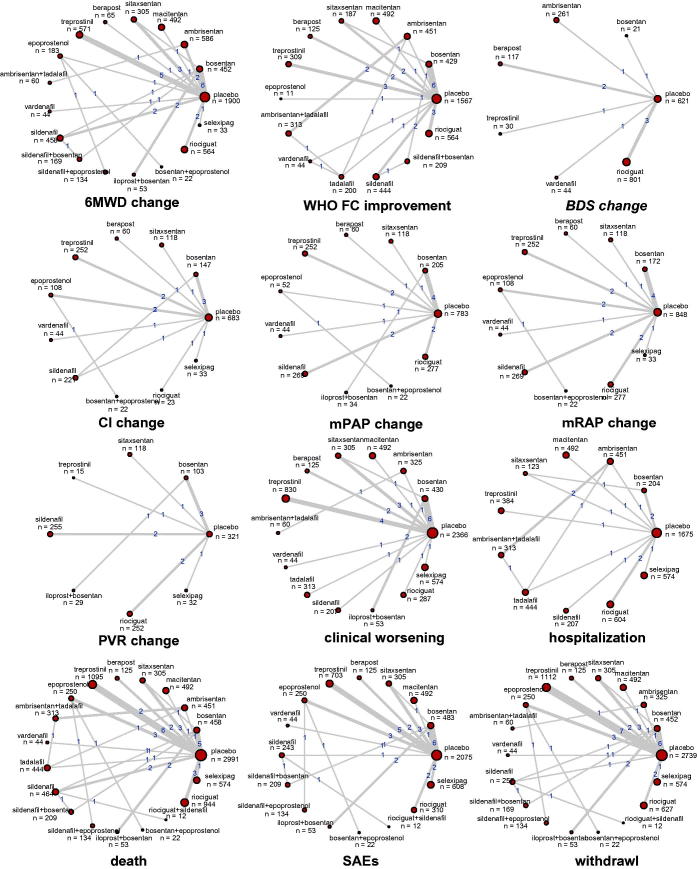
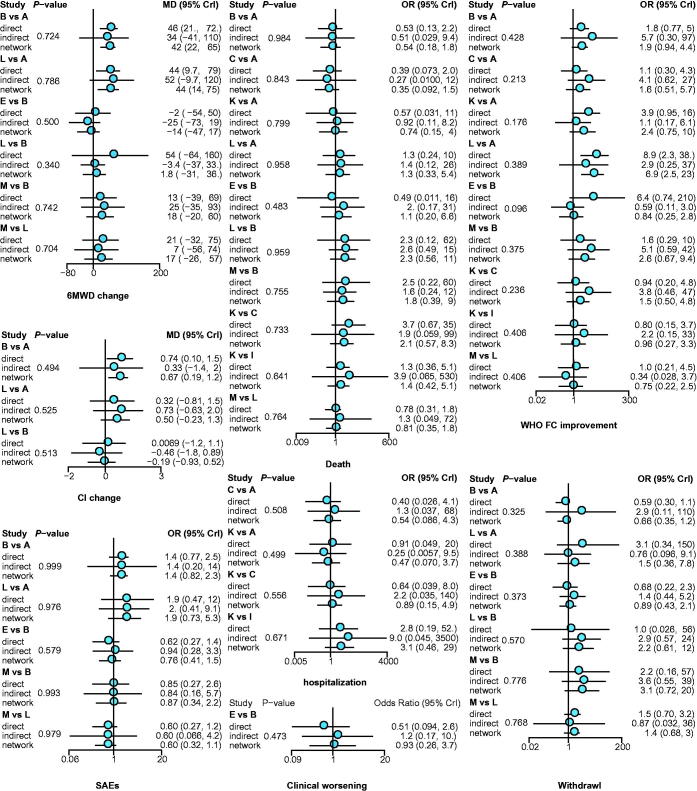
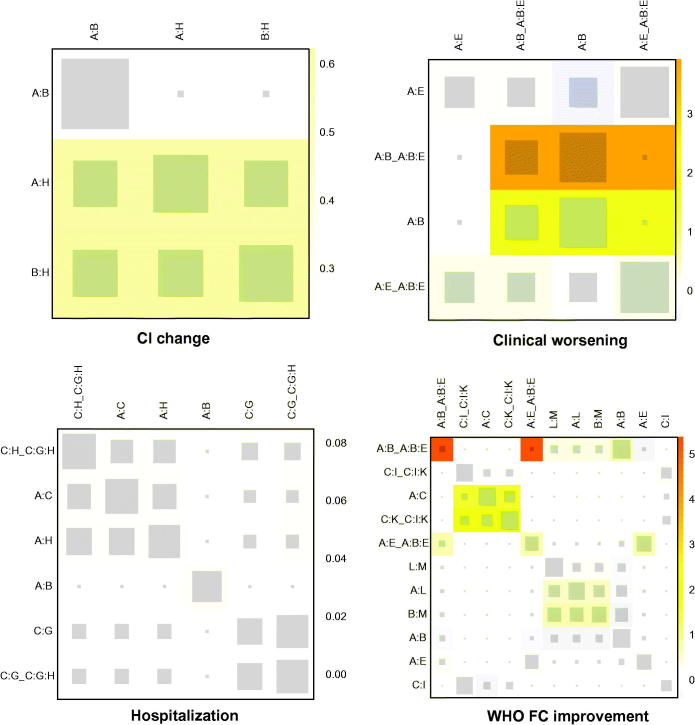
Pulmonary arterial hypertension (PAH) can be relieved by pharmacological interventions, especially the targeted drug, which is classified into endothelin receptor antagonist, phosphodiesterase 5 inhibitor, prostaglandin I, soluble guanylate cyclase stimulator and selective non-prostanoid prostacyclin receptor agonist. To solve the contradictions existing in reported trials and provide a comprehensive guideline for clinical practice. PubMed, Embase, Cochrane library, and clinicaltrials.gov were searched. The basic information about the article, trial, arm, intervention, and the detailed data of outcome, including 6 minutes walking distance (6MWD) change, WHO functional class (FC) improvement, Borg dyspnea score (BDS) change, cardiac index (CI) change, mean pulmonary arterial pressure (mPAP) change, mean right arterial pressure (mRAP) change, pulmonary vascular resistance (PVR) change, clinical worsening, hospitalization, death, severe adverse events (SAEs), and withdrawal were extracted. The rank of treatments was estimated. 10,230 cases provided the firsthand comparison data about targeted drugs for treating PAH. For 6MWD, ambrisentan + tadalafil, vardenafil, and sildenafil + bosentan were better than others. Epoprostenol, macitentan, and sildenafil represented a greater WHO FC improvement. Vardenafil and treprostinil were better for BDS. So were bosentan + epoprostenol and bosentan alone for CI. Iloprost plus bosentan, bosentan + epoprostenol, and epoprostenol were better for mPAP. Iloprost plus bosentan, bosentan alone, and selexipag could reduce PVR. Sildenafil, epoprostenol, and vardenafil had the highest probability to reduce the incidence of death and withdrawal. To conclude, vardenafil and iloprost + bosentan showed relatively better performance in both efficacy and safety. However, the therapeutic choice should be made according to both the feature of each therapy and the individual condition.
肺动脉高压(PAH)可以通过药物干预得到缓解,特别是靶向药物,它可分为内皮素受体拮抗剂、磷酸二酯酶 5 抑制剂、前列环素 I、可溶性鸟苷酸环化酶刺激剂和选择性非前列腺素类前列环素受体激动剂。为了解决报道的试验中存在的矛盾,并为临床实践提供全面的指南。检索了 PubMed、Embase、Cochrane 图书馆和 clinicaltrials.gov。提取了文章、试验、臂、干预以及结局的详细数据的基本信息,包括 6 分钟步行距离(6MWD)变化、世界卫生组织(WHO)功能分级(FC)改善、Borg 呼吸困难评分(BDS)变化、心指数(CI)变化、平均肺动脉压(mPAP)变化、平均右心房压(mRAP)变化、肺血管阻力(PVR)变化、临床恶化、住院、死亡、严重不良事件(SAEs)和退出。治疗的等级进行了估计。10230 例提供了靶向药物治疗 PAH 的直接比较数据。在 6MWD 方面,安贝生坦+他达拉非、伐地那非和西地那非+波生坦优于其他药物。依前列醇、马西替坦和西地那非代表 WHO FC 改善更大。伐地那非和曲前列尼尔对 BDS 更好。波生坦+依前列醇和波生坦单独使用对 CI 更好。伊洛前列素+波生坦、波生坦+依前列醇和依前列醇对 mPAP 更好。伊洛前列素+波生坦、波生坦单独使用和塞来昔帕可降低 PVR。西地那非、依前列醇和伐地那非降低死亡率和退出率的概率最高。总之,伐地那非和伊洛前列素+波生坦在疗效和安全性方面表现相对较好。然而,治疗选择应根据每种治疗方法的特点和个体情况来做出。