Department of Respiratory and Critical Care Medicine, Beijing Institute of Respiratory Medicine, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, China.
Department of Respiratory and Critical Care Medicine, Beijing Institute of Respiratory Medicine, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, China.
J Crit Care. 2019 Apr;50:1-10. doi: 10.1016/j.jcrc.2018.10.033. Epub 2018 Nov 3.
To determine if recruitment manoeuvres (RMs) would decrease 28-day mortality of patients with acute respiratory distress syndrome (ARDS) compared with standard care.
Relevant randomized controlled trials (RCTs) published prior to April 26, 2018 were systematically searched. The primary outcome was mortality. The secondary outcomes were oxygenation, barotrauma or pneumothorax, the need for rescue therapies. Data were pooled using the random effects model. And the quality of evidence was assessed by the GRADE system.
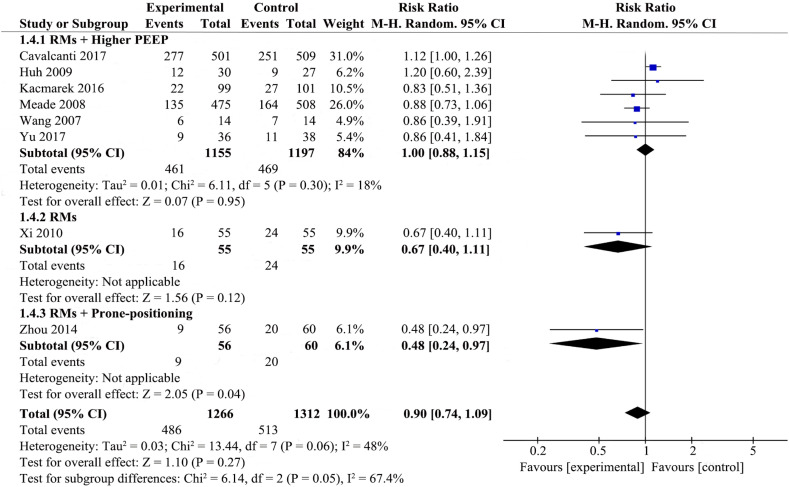
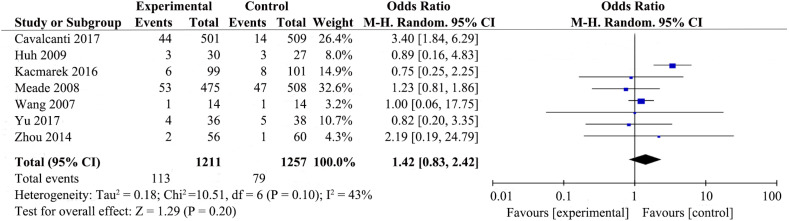
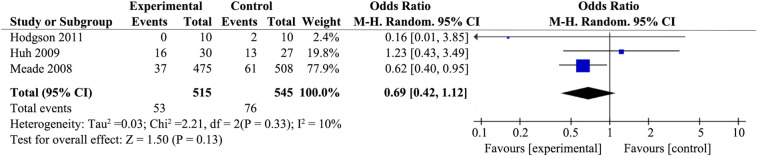
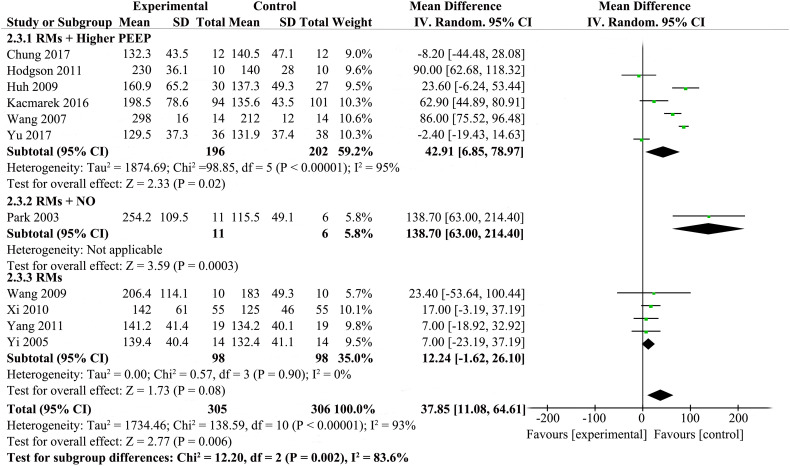
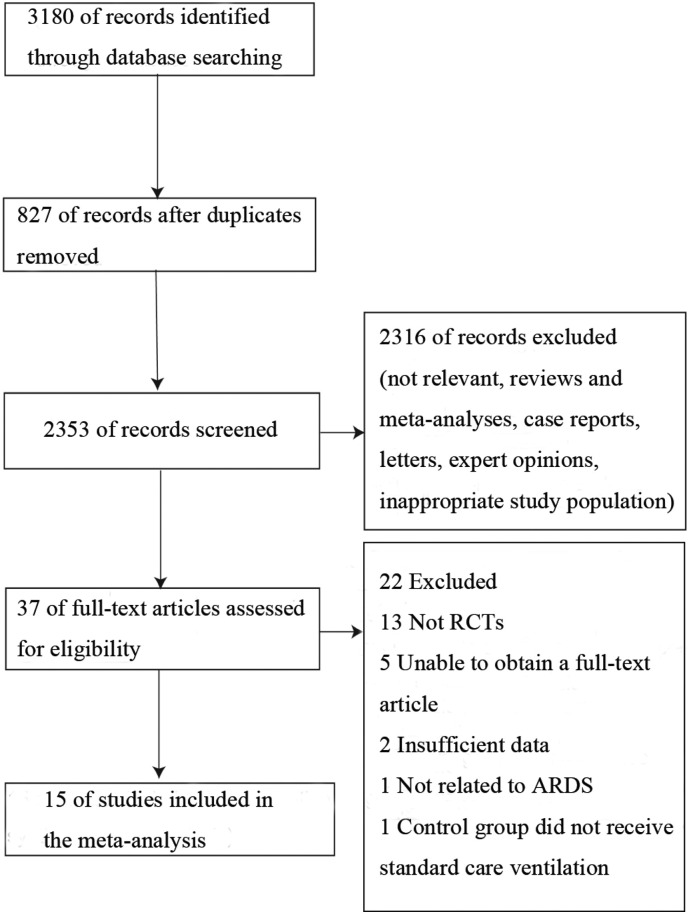
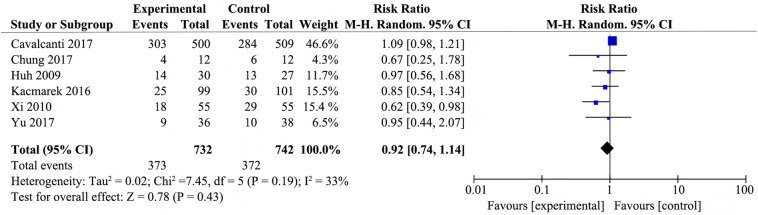
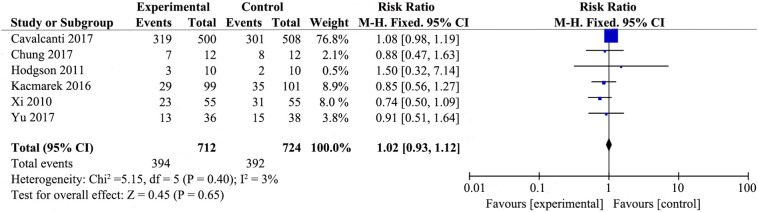
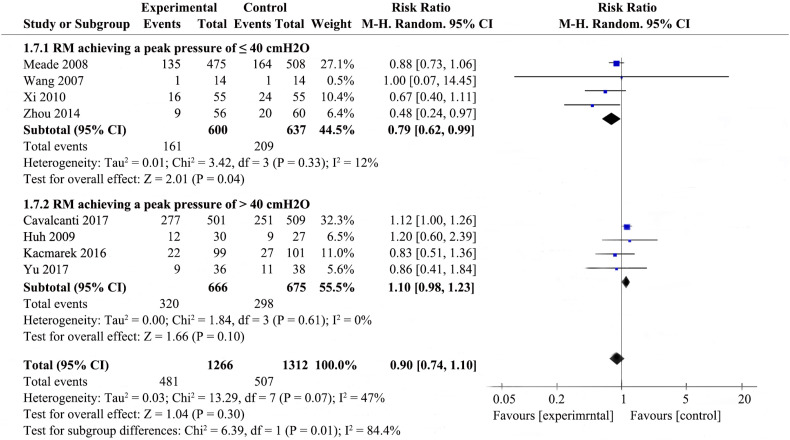
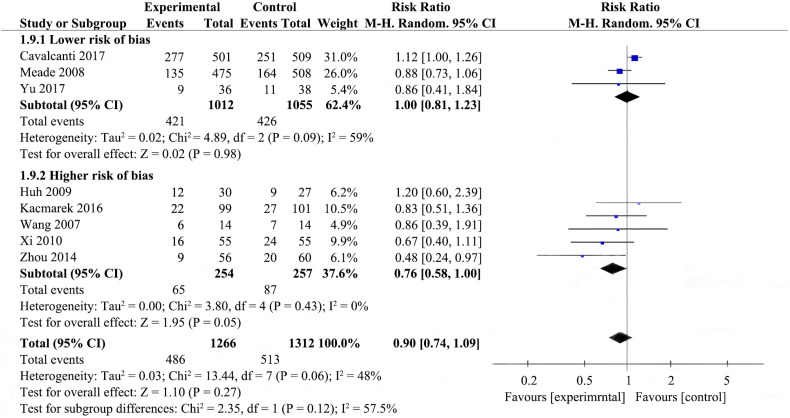
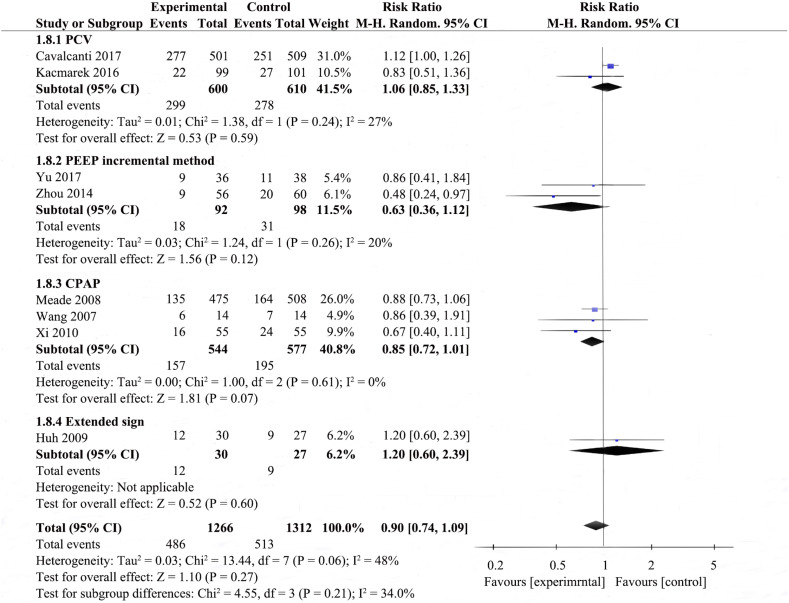
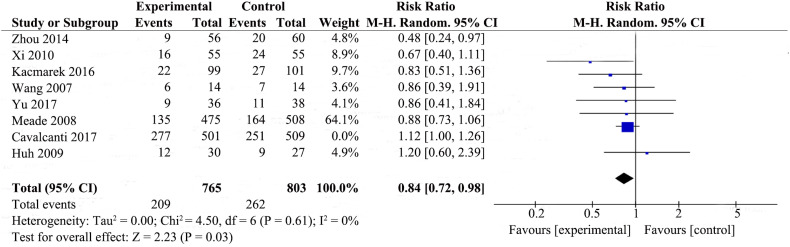
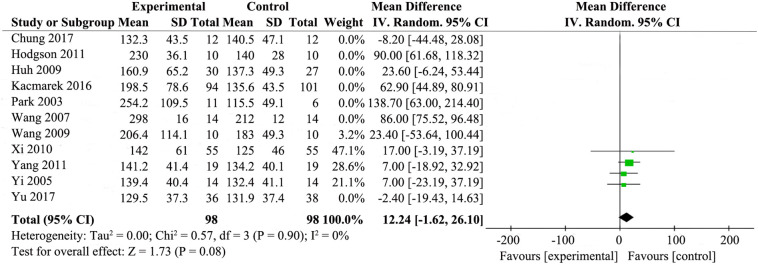
Of 3180 identified studies, 15 were eligibly included in our analysis (N = 2755 participants). In the primary outcome, RMs were not associated with reducing 28-day mortality (RR 0.90; 95% CI 0.74-1.09), ICU mortality (RR 0.92; 95% CI 0.74-1.1), and the in-hospital mortaliy (RR 1.02; 95% CI 0.93-1.12). In the secondary outcomes, RMs could improve oxygenation (MD 37.85; 95% CI 11.08-64.61), the rates of barotrauma (RR 1.42; 95% CI 0.83-2.42) and the need for rescue therapies (RR 0.69; 95% CI 0.42-1.12) did not show any difference in the ARDS patients with RMs.
Earlier meta-analyses found decreased mortality with RMs, in the contrary, our results indicate that RMs could improve oxygenation without detrimental effects, but it does not appear to reduce mortality.
确定与标准治疗相比,募集手法(RM)是否会降低急性呼吸窘迫综合征(ARDS)患者 28 天的死亡率。
系统检索了截至 2018 年 4 月 26 日之前发表的相关随机对照试验(RCT)。主要结局为死亡率。次要结局为氧合、气压伤或气胸、需要抢救治疗。使用随机效应模型汇总数据。使用 GRADE 系统评估证据质量。
在 3180 项已识别的研究中,有 15 项符合纳入标准,纳入本分析(N=2755 名参与者)。在主要结局方面,RM 与降低 28 天死亡率(RR 0.90;95%CI 0.74-1.09)、ICU 死亡率(RR 0.92;95%CI 0.74-1.1)和住院死亡率(RR 1.02;95%CI 0.93-1.12)无关。在次要结局方面,RM 可改善氧合(MD 37.85;95%CI 11.08-64.61),气压伤发生率(RR 1.42;95%CI 0.83-2.42)和需要抢救治疗(RR 0.69;95%CI 0.42-1.12)的比例在 RM 治疗的 ARDS 患者中没有差异。
早期荟萃分析发现 RM 可降低死亡率,但我们的结果表明,RM 可改善氧合而无不良影响,但似乎不会降低死亡率。