Puymirat Etienne, Bonaca Marc, Fumery Maxime, Tea Victoria, Aissaoui Nadia, Lemesles Gilles, Bonello Laurent, Ducrocq Grégory, Cayla Guillaume, Ferrières Jean, Schiele François, Simon Tabassome, Danchin Nicolas
Department of Cardiology, Hôpital Européen Georges Pompidou (HEGP), Assistance Publique-Hôpitaux de Paris (AP-HP), Paris, France.
Division of Cardiovascular Medicine, TIMI Study Group, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts.
Clin Cardiol. 2019 Feb;42(2):227-234. doi: 10.1002/clc.23131. Epub 2018 Dec 27.
Guidelines recommend using risk stratification tools in acute myocardial infarction (AMI) to assist decision-making. The Thrombolysis in Myocardial Infarction Risk Score for Secondary Prevention (TRS-2P) has been recently developed to characterize long-term risk in patients with MI.
We aimed to assess the TRS-2P in the French Registry of Acute ST Elevation or non-ST elevation MI registries.
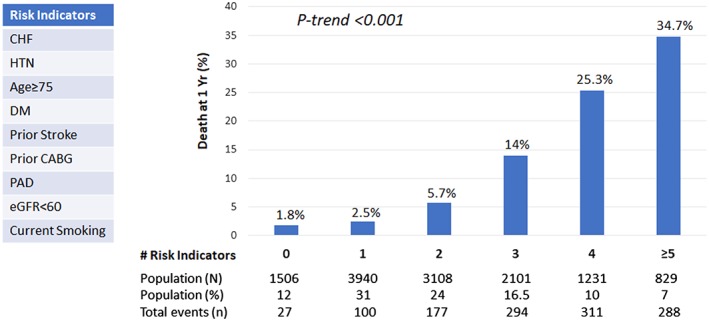
We used data from three 1-month French registries, conducted 5 years apart, from 2005 to 2015, including 13 130 patients with AMI (52% ST-elevation myocardial infarction [STEMI]). Atherothrombotic risk stratification was performed using the TRS-2P score. Patients were divided in to three categories: G1 (low-risk, TRS-2P = 0/1); G2 (intermediate-risk, TRS-2P = 2); and G3 (high-risk, TRS-2P ≥ 3). Baseline characteristics and outcomes were analyzed according to TRS-2P categories.
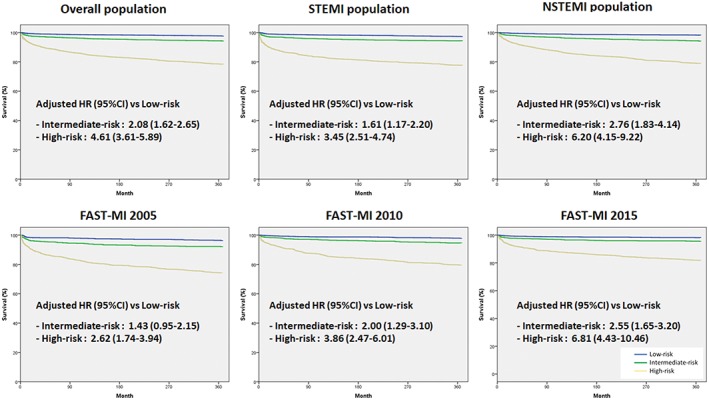
A total of 12 715 patients (in whom TRS-2P was available) were included. Prevalence of G1, G2, and G3 was 43%, 24%, and 33% respectively. Clinical characteristics and management significantly differed according to TRS-2P categories. TRS-2P successfully defined residual risk of death at 1 year (C-statistic 0.78): 1-year survival was 98% in G1, 94% in G2, and 78.5% in G3 (P < 0.001). Using Cox multivariate analysis, G3 was independently associated with higher risk of death at 1 year (hazard ratio [HR] 4.61; 95% confidence interval [CI]: 3.61-5.89), as G2 (HR 2.08; 95% CI: 1.62-2.65) compared with G1. The score appeared robust and correlated well with mortality in STEMI and NSTEMI populations, as well as in each cohort separately.
The TRS-2P appears to be a robust risk score, identifying patients at high risk after AMI irrespective of the type of MI and historical period.
指南建议在急性心肌梗死(AMI)中使用风险分层工具来辅助决策。最近开发了心肌梗死二级预防溶栓风险评分(TRS - 2P)以描述心肌梗死患者的长期风险。
我们旨在评估法国急性ST段抬高或非ST段抬高心肌梗死注册研究中的TRS - 2P。
我们使用了来自法国三个为期1个月的注册研究的数据,这些研究在2005年至2015年期间相隔5年进行,包括13130例AMI患者(52%为ST段抬高型心肌梗死[STEMI])。使用TRS - 2P评分进行动脉粥样硬化血栓形成风险分层。患者分为三类:G1(低风险,TRS - 2P = 0/1);G2(中风险,TRS - 2P = 2);G3(高风险,TRS - 2P≥3)。根据TRS - 2P类别分析基线特征和结局。
共纳入12715例患者(可获得TRS - 2P)。G1、G2和G3的患病率分别为43%、24%和33%。临床特征和管理根据TRS - 2P类别有显著差异。TRS - 2P成功定义了1年时的死亡残余风险(C统计量0.78):G1组1年生存率为98%,G2组为94%,G3组为78.5%(P < 0.001)。使用Cox多变量分析,与G1组相比,G3组在1年时独立与更高的死亡风险相关(风险比[HR] 4.61;95%置信区间[CI]:3.61 - 5.89),G2组也是如此(HR 2.08;95% CI:1.62 - 2.65)。该评分似乎很稳健,并且与STEMI和NSTEMI人群以及每个队列单独的死亡率相关性良好。
TRS - 2P似乎是一个稳健的风险评分,可识别AMI后高危患者,无论心肌梗死类型和历史时期如何。