van Westen Els, Knol Mirjam J, Wijmenga-Monsuur Alienke J, Tcherniaeva Irina, Schouls Leo M, Sanders Elisabeth A M, van Els Cecile A C M, Berbers Guy A M, Rots Nynke Y
Center for Infectious Disease Control, National Institute for Public Health and the Environment, 3720 BA Bilthoven, The Netherlands.
Vaccines (Basel). 2018 Dec 11;6(4):82. doi: 10.3390/vaccines6040082.
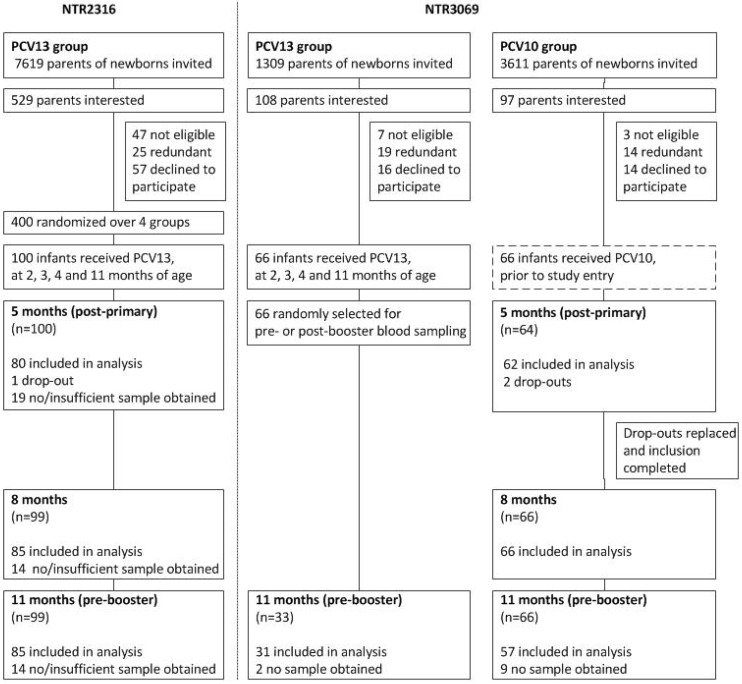
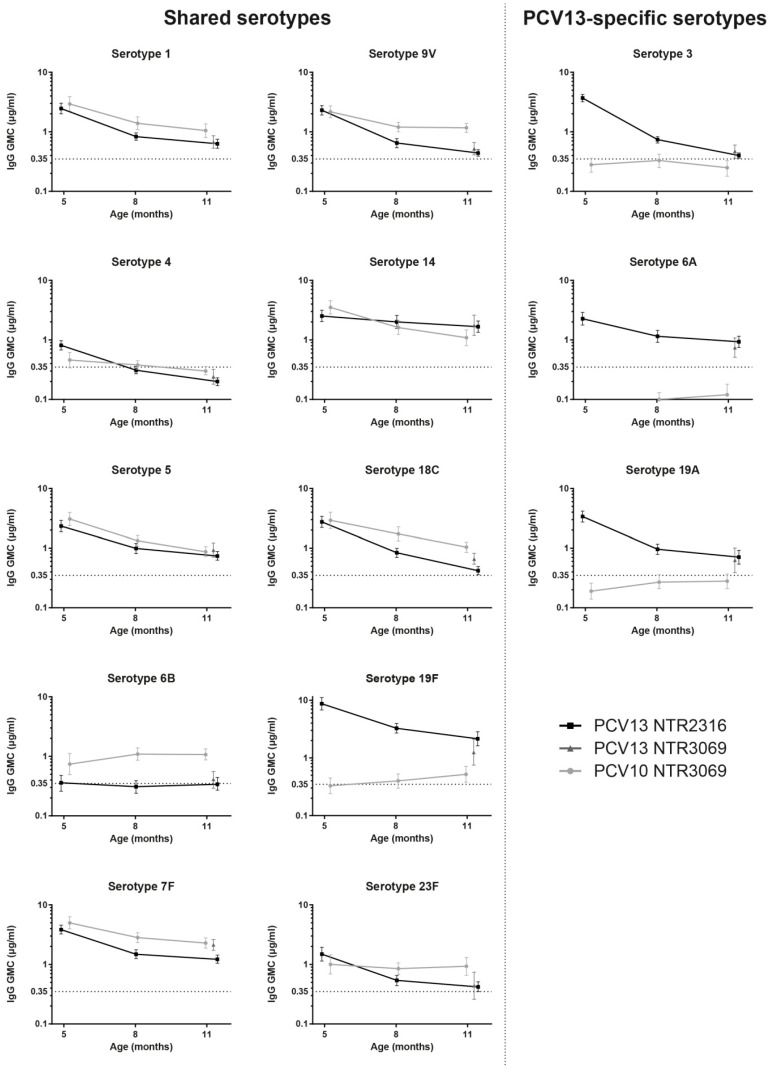
The two currently available ten- and thirteen-valent pneumococcal conjugate vaccines (PCV10 and PCV13) both induce serotype-specific IgG anti-polysaccharide antibodies and are effective in preventing vaccine serotype induced invasive pneumococcal disease (IPD) as well as in reducing overall vaccine-serotype carriage and transmission and thereby inducing herd protection in the whole population. IgG levels decline after vaccination and could become too low to prevent carriage acquisition and/or pneumococcal disease. We compared the levels of 10-valent (PCV10) and 13-valent (PCV13) pneumococcal vaccine induced serum IgG antibodies at multiple time points after primary vaccinations. Data from two separate studies both performed in the Netherlands in infants vaccinated at 2, 3, and 4 months of age with either PCV10 or PCV13 were compared. Antibody levels were measured at 5, 8, and 11 months of age, during the interval between the primary immunization series and the 11-months booster dose. Serotype-specific IgG levels were determined by multiplex immunoassay. Although antibody kinetics showed significant variation between serotypes and between vaccines for the majority of the 10 shared serotypes, i.e., 1, 5, 7F, 9V, 14, 18C, and 23F, antibody concentrations were sufficiently high for both vaccines, immediately after the primary series and throughout the whole period until the booster dose. In contrast, for serotypes 4 and 19F in the PCV10 group and for serotypes 4 and 6B in the PCV13 group, IgG antibody concentrations already come within reach of the frequently used seroprotection level of 0.35 μg/mL immediately after the primary series at the five month time point and/or at eight months. This paper addresses the importance of revealing differences in serotype-specific and pneumococcal vaccine-dependent IgG antibody patterns during the interval between the primary series and the booster dose, an age period with a high IPD incidence. Trial registration: www.trialregister.nl NTR3069 and NTR2316.
目前可用的两种十价和十三价肺炎球菌结合疫苗(PCV10和PCV13)均能诱导血清型特异性IgG抗多糖抗体,在预防疫苗血清型引起的侵袭性肺炎球菌疾病(IPD)以及减少总体疫苗血清型携带和传播方面有效,从而在整个人口中诱导群体保护。接种疫苗后IgG水平会下降,可能会降至过低水平,无法预防携带感染和/或肺炎球菌疾病。我们比较了在初次接种疫苗后的多个时间点,十价(PCV10)和十三价(PCV13)肺炎球菌疫苗诱导的血清IgG抗体水平。比较了在荷兰进行的两项独立研究的数据,这两项研究均针对2、3、4月龄接种PCV10或PCV13的婴儿。在5、8和11月龄时测量抗体水平,即在初次免疫系列和11月龄加强剂量之间的间隔期。通过多重免疫测定法测定血清型特异性IgG水平。尽管对于大多数10种共同血清型(即1、5、7F、9V、14、18C和23F),抗体动力学在血清型之间以及疫苗之间显示出显著差异,但在初次系列接种后直至加强剂量的整个期间,两种疫苗的抗体浓度都足够高。相比之下,对于PCV10组中的血清型4和19F以及PCV13组中的血清型4和6B,在5个月时间点和/或8个月时,初次系列接种后IgG抗体浓度立即达到常用的血清保护水平0.35μg/mL。本文阐述了在初次系列接种和加强剂量之间的间隔期(这是IPD发病率较高的年龄段)揭示血清型特异性和肺炎球菌疫苗依赖性IgG抗体模式差异的重要性。试验注册:www.trialregister.nl NTR3069和NTR2316。