Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, UK.
Centre for Cognitive Ageing and Cognitive Epidemiology, Department of Psychology, University of Edinburgh, Edinburgh, UK.
J Neurol Neurosurg Psychiatry. 2019 Apr;90(4):436-443. doi: 10.1136/jnnp-2018-319134. Epub 2018 Dec 15.
Many studies examining stroke outcomes focus on more severe strokes or have short follow-up periods, so the long-term outcomes post-minor ischaemic stroke are unclear.
We recruited participants from inpatient and outpatient services with a lacunar or minor cortical ischaemic stroke (National Institutes of Health Stroke Scale score <8) and assessed current and premorbid cognitive functioning (Addenbrooke's Cognitive Examination-Revised (ACE-R), National Adult Reading Test (NART)), physical functioning (Timed Get Up and Go (TUG), 9-Hole Peg Test (9HPT)), dependency (modified Rankin Scale (mRS)), depression (Beck's Depression Inventory) in-person and remotely (Stroke Impact Scale).
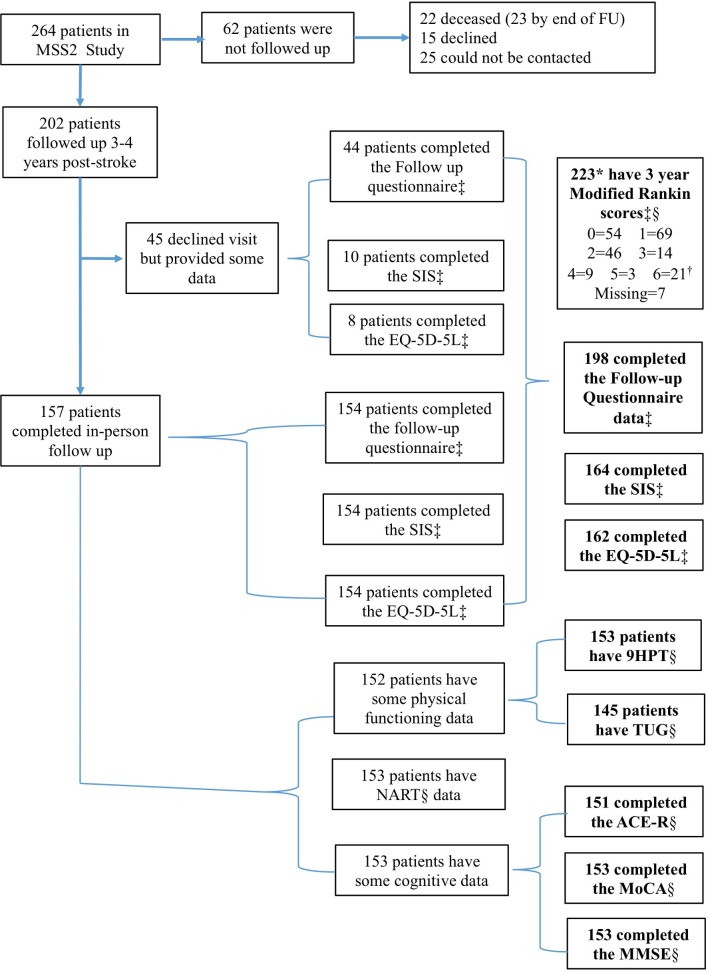
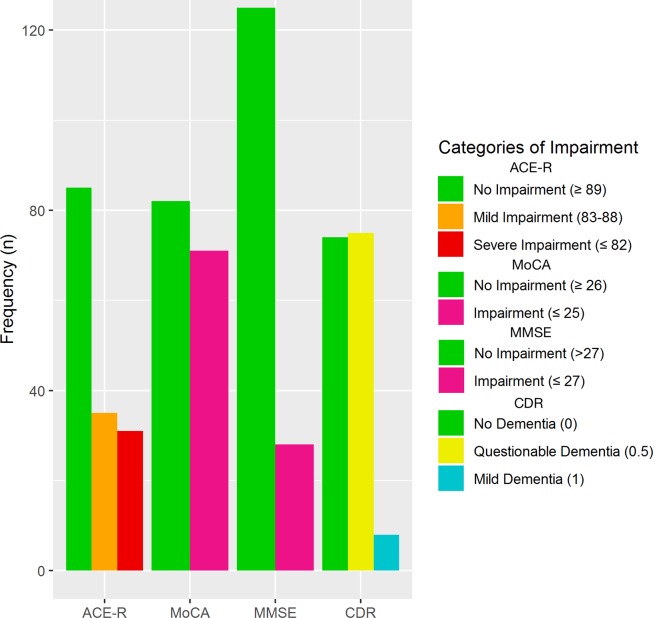
We followed up 224/264 participants at 3 years (mean age at index stroke=67, 126 (56%) men, 25 non-contactable, 15 declined): 66/151 (44%) had cognitive impairment, mean ACE-R 88 (SD 9, range 54-100/100), 61/156 (39%) had depression and 26/223 (12%) were dependent (mRS=3-5). Cognitive impairment at 3 years affected all ACE-R subdomains and was associated with ACE-R 1 year (β=1.054, p<0.001) and NART (β=1.023, p<0.05). Poor physical function was associated with stroke severity (TUG, β=1.064, p<0.01) and recurrent stroke (9HPT, β=1.130, p<0.05 right, β=1.214, p<0.05 left). Higher ACE-R scores were associated with faster TUG (β=-0.279, p<0.05) and 9HPT (right β=-0.257, p<0.05; left β=-0.302, p=0.05) and inversely with dependency (mRS=3-5, OR 0.88, 95% CI 0.80 to 0.97). We adjusted analyses for demographic, stroke and known risk factors. In-person and remote assessments were highly correlated.
Cognitive, physical impairments and depression are common and interrelated 3 years after minor stroke. Cognitive and physical impairments require rehabilitation after minor stroke and argue for better integration of stroke and dementia services.
许多研究检查中风结果侧重于更严重的中风或随访时间短,因此,轻微缺血性中风后的长期结果尚不清楚。
我们从住院和门诊服务中招募了腔隙性或小皮质性缺血性中风(国立卫生研究院中风量表评分<8)患者,并评估了当前和发病前的认知功能(改良的 Addenbrooke 认知测验修订版(ACE-R)、全国成人阅读测验(NART))、身体功能(计时起身行走测试(TUG)、9 孔钉测试(9HPT))、依赖性(改良 Rankin 量表(mRS))、抑郁(贝克抑郁量表),面对面和远程评估(中风影响量表)。
我们在 3 年时对 264 名参与者中的 224 名进行了随访(指数中风时的平均年龄为 67 岁,126 名男性(56%),25 名无法联系,15 名拒绝):66/151 名(44%)有认知障碍,ACE-R 平均得分为 88(标准差 9,范围 54-100/100),61/156 名(39%)有抑郁,26/223 名(12%)依赖(mRS=3-5)。3 年后的认知障碍影响所有 ACE-R 子域,与 ACE-R 1 年(β=1.054,p<0.001)和 NART(β=1.023,p<0.05)相关。身体功能不良与中风严重程度(TUG,β=1.064,p<0.01)和复发性中风(9HPT,β=1.130,p<0.05 右侧,β=1.214,p<0.05 左侧)相关。较高的 ACE-R 评分与 TUG(β=-0.279,p<0.05)和 9HPT(右侧β=-0.257,p<0.05;左侧β=-0.302,p=0.05)的速度较快相关,与依赖性(mRS=3-5,OR 0.88,95%CI 0.80-0.97)呈负相关。我们对人口统计学、中风和已知危险因素进行了分析调整。面对面和远程评估高度相关。
轻微中风后 3 年,认知、身体损伤和抑郁较为常见且相互关联。中风后需要对认知和身体损伤进行康复,这就需要更好地整合中风和痴呆症服务。