Sohail Ghania, Xu Xiaoyu, Christman Mary C, Tompkins Thomas A
Lallemand Health Solutions Inc., Montreal, QC H4P 2R2, Canada.
MCC Statistical Consulting, Gainesville, FL 32605, United States.
World J Clin Cases. 2018 Dec 6;6(15):961-984. doi: 10.12998/wjcc.v6.i15.961.
To assess the effects of probiotic Medilac-S as adjunctive therapy for the induction of remission of ulcerative colitis (UC) in a Chinese population through a systematic review and meta-analysis.
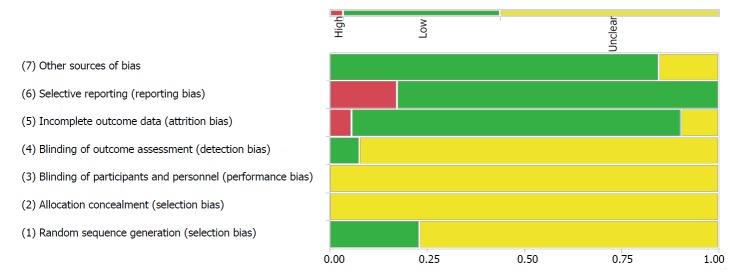
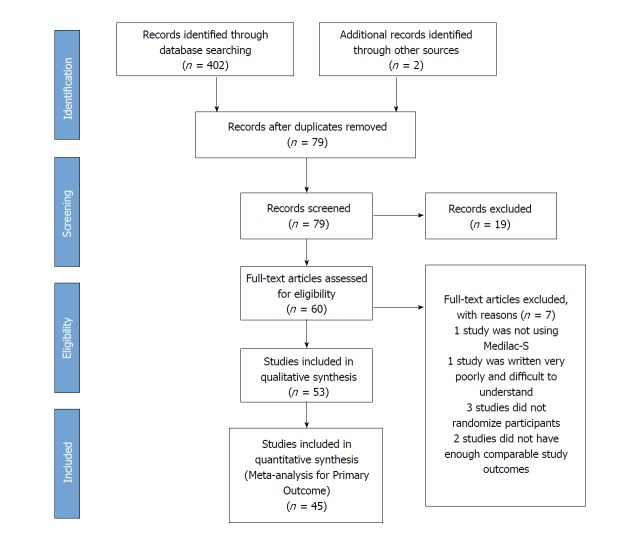
A systematic literature search was conducted to find randomized, controlled trials in a Chinese population with at least two study arms - a control arm which receives a conventional, oral aminosalicylate drug, and a treatment arm, which administers the same conventional drug in conjunction with the probiotic Medilac-S . Both English and Chinese databases were searched, including PubMed, EMBASE, Google Scholar, Chinese National Knowledge Infrastructure, Wanfang Data, and VIP Search, and study data was extracted onto standardized abstraction sheets. Meta-analyses were conducted for primary and secondary outcomes of interest using a fixed or random effects model. The primary outcome was the induction of clinical remission and the secondary outcomes included changes in Sutherland index, endoscopic and histological scores, proportion of reported clinical symptoms and adverse events (AEs). For outcomes with sufficient data, the type of conventional drug therapy was also assessed to determine if the effects of combination therapy with Medilac-S was influenced by drug type. All tests were conducted using a type I error rate of 0.05 and all confidence intervals (CI) were based on a 95% confidence level. Review protocol was uploaded to PROSPERO (CRD42018085658 upon completion).
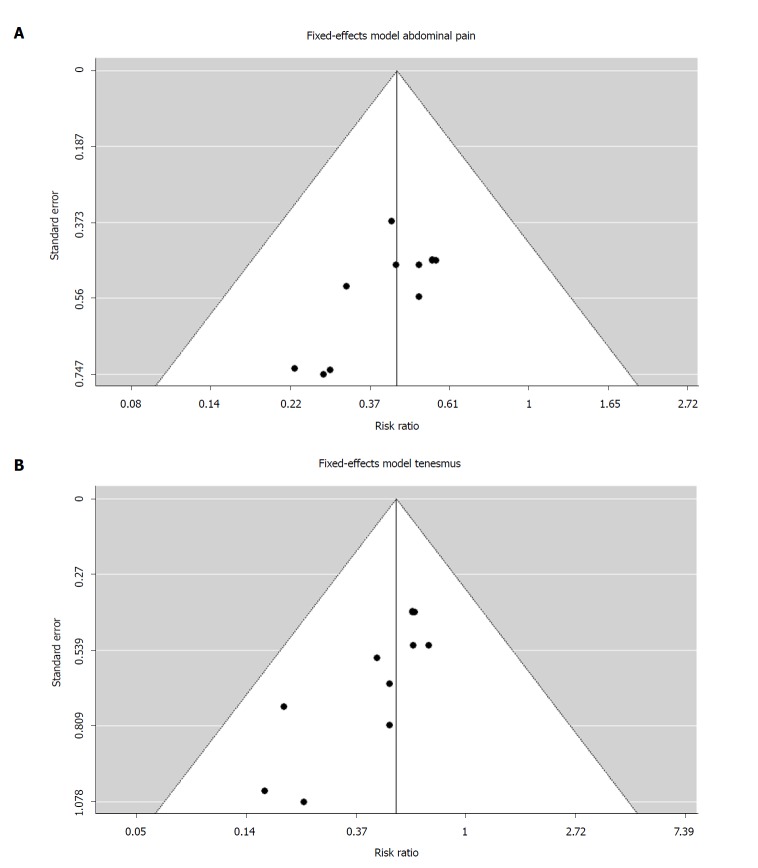
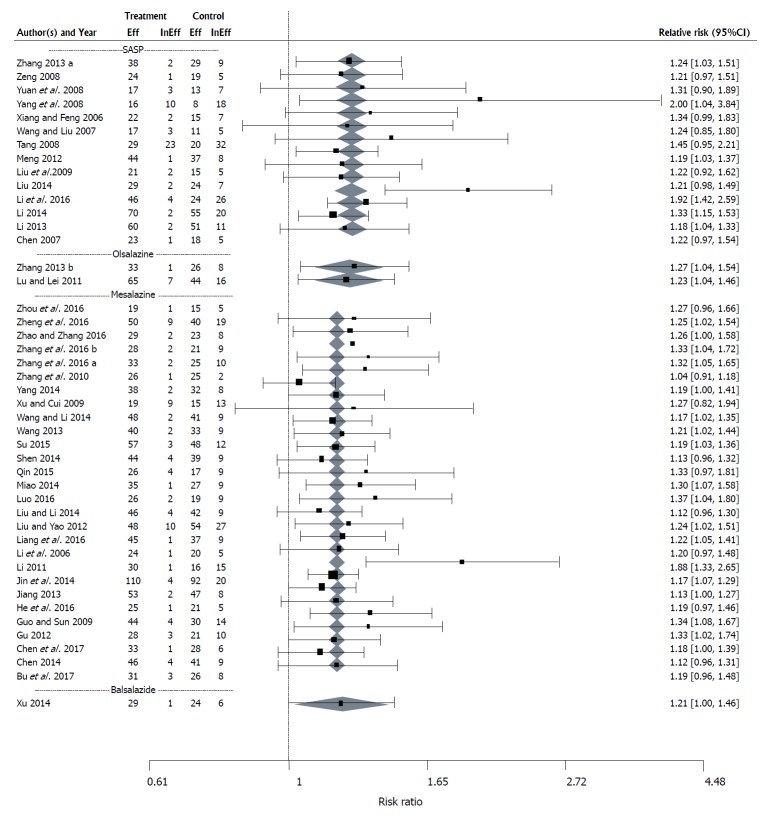
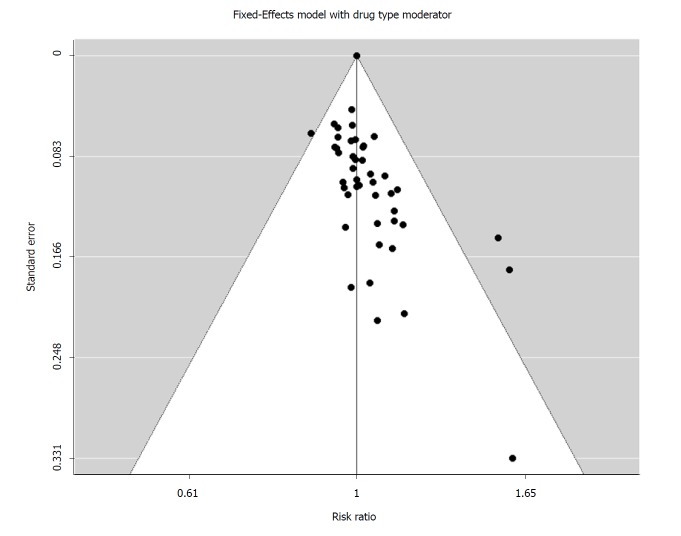
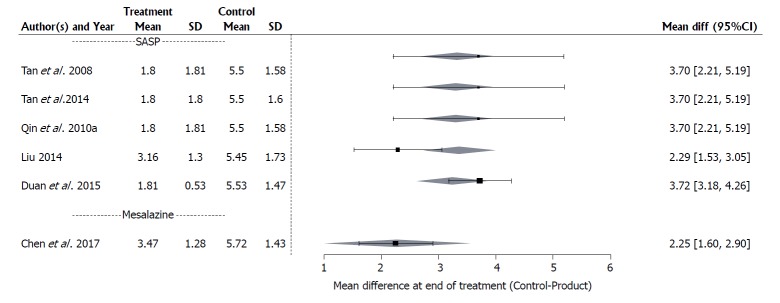
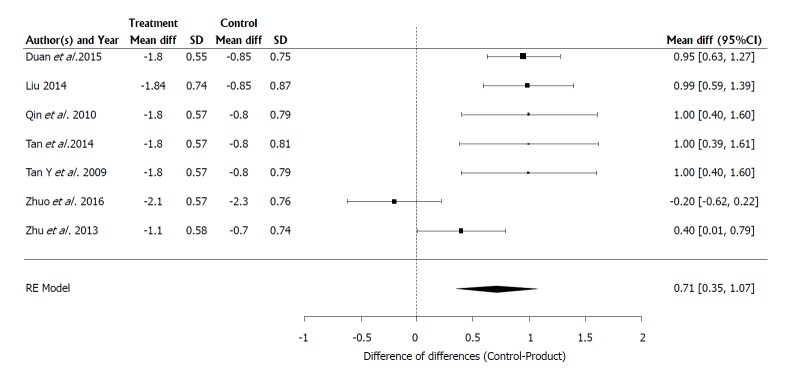
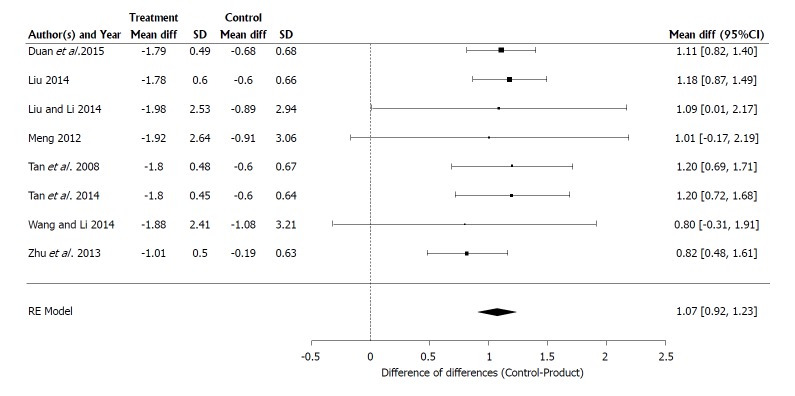
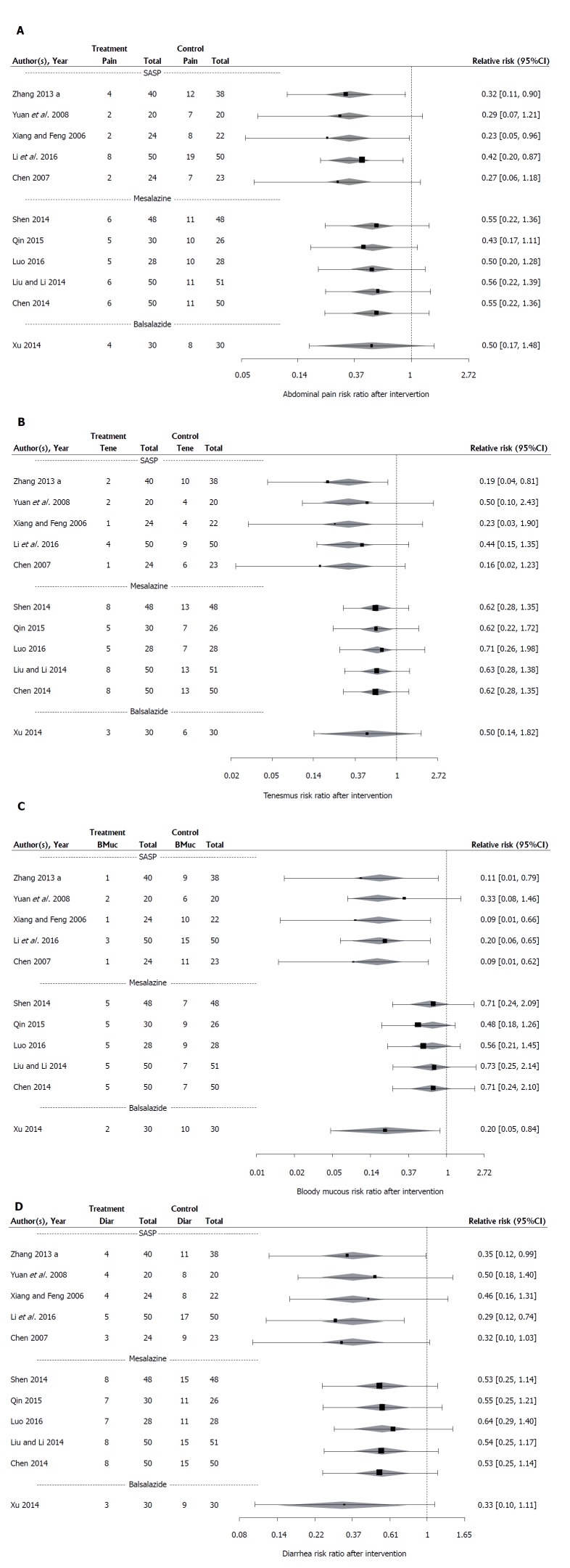
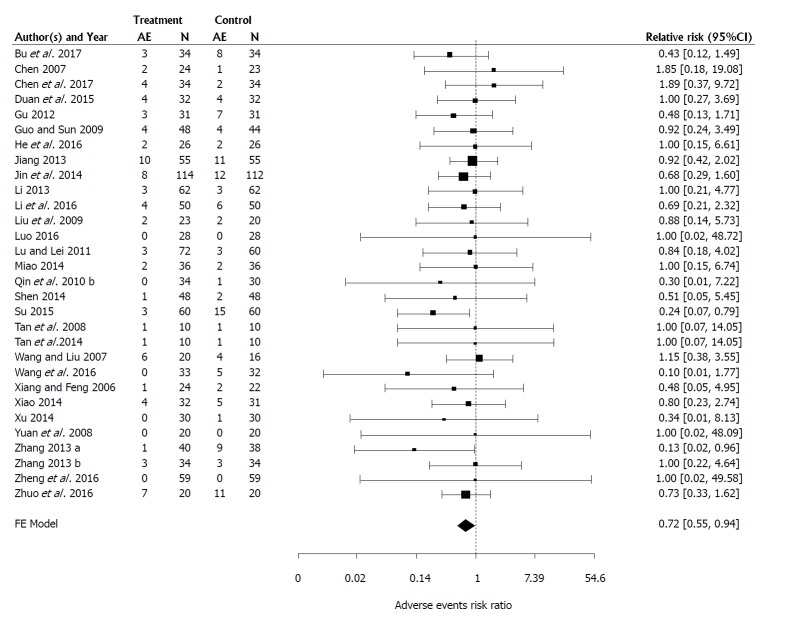
Fifty-three clinical trials with a total of 3984 participants were identified and included in the review. Medilac-S adjunctive therapy significantly improved induction of clinical remission (RR = 1.21; 95%CI: 1.18-1.24; < 0.0001) with the estimated likelihood of effective treatment, on average, 21% higher for those consuming the probiotic. Sutherland index scores showed the control mean was on average 3.10 (CI: 2.41-3.78; = 0.0428) units greater than the treatment mean, thereby demonstrating significant improvement in participants taking the probiotic. Similarly, a significant difference was seen between the overall reduction of endoscopic and histological scores of control and treatment arm participants, with score decreases in the control groups 0.71 (CI: 0.3537-1.0742) and 1.1 (CI: 0.9189-1.2300) units smaller than treatment group score decreases. The proportion of participants reporting clinical symptoms, (abdominal pain, tenesmus, blood and mucous in stool, and diarrhea) was significantly reduced after combination therapy with Medilac-S ( < 0.0001) and estimated to be on average 44% (RR = 0.44, CI: 0.32-0.59), 53% (RR = 0.53, CI: 0.38-74), 40% (RR = 0.40, CI: 0.28-0.58) and 47% (RR = 0.47 CI: 0.36-0.42) respectively, of the proportion of individuals reporting the aforementioned symptoms after conventional therapy alone. The risk of AEs was also significantly reduced with adjunctive Medilac-S therapy. The proportion of individuals in the treatment groups reporting AEs was an estimated 72% of the proportion of individuals in the control groups reporting AEs (RR = 0.72, CI: 0.55-0.94, = 0.0175). Upon comparing effect means for different drug types in conjunction with Medilac-S, evidence of significant variability ( < 0.0001) was observed, and sulfasalazine was found to be the most effective drug in both primary and secondary outcomes.
Evidence suggests Medilac-S adjunctive therapy should be considered standard care for UC in a Chinese population because it aids in the induction of clinical remission, improves symptoms of the gastrointestinal tract and reduces risk of AEs.
通过系统评价和荟萃分析,评估益生菌美常安作为辅助疗法在中国人群中诱导溃疡性结肠炎(UC)缓解的效果。
进行系统的文献检索,以查找在中国人群中进行的随机对照试验,该试验至少有两个研究组——一个对照组接受传统口服氨基水杨酸药物,一个治疗组在使用相同传统药物的同时联合使用益生菌美常安。检索了英文和中文数据库,包括PubMed、EMBASE、谷歌学术、中国知网、万方数据和维普资讯,并将研究数据提取到标准化的摘要表上。使用固定或随机效应模型对感兴趣的主要和次要结局进行荟萃分析。主要结局是诱导临床缓解,次要结局包括萨瑟兰指数变化、内镜和组织学评分、报告的临床症状比例和不良事件(AE)。对于有足够数据的结局,还评估了传统药物治疗的类型,以确定美常安联合治疗的效果是否受药物类型影响。所有检验的I型错误率为0.05,所有置信区间(CI)基于95%置信水平。审查方案已上传至PROSPERO(完成后为CRD42018085658)。
共识别出53项临床试验,总计3984名参与者,并纳入本综述。美常安辅助治疗显著提高了临床缓解的诱导率(RR = 1.21;95%CI:1.18 - 1.24;P < 0.0001),服用益生菌的患者有效治疗的估计可能性平均高21%。萨瑟兰指数评分显示,对照组的平均得分比治疗组平均得分高3.10(CI:2.41 - 3.78;P = 0.0428)个单位,从而表明服用益生菌的参与者有显著改善。同样,对照组和治疗组参与者内镜和组织学评分的总体降低之间存在显著差异,对照组评分降低比治疗组分别小0.71(CI:0.3537 - 1.0742)和1.1(CI:0.9189 - 1.2300)个单位。联合美常安治疗后,报告临床症状(腹痛、里急后重、便血和黏液便、腹泻)的参与者比例显著降低(P < 0.0001),估计分别平均为单独接受传统治疗后报告上述症状的个体比例的44%(RR = 0.44,CI:0.32 - 0.59)、53%(RR = 0.53,CI:0.38 - 74)、40%(RR = 0.40,CI:0.28 - 0.58)和47%(RR = 0.47,CI:0.36 - 0.42)。美常安辅助治疗也显著降低了AE风险。治疗组报告AE的个体比例估计为对照组报告AE个体比例的72%(RR = 0.72,CI:0.55 - 0.94,P = 0.0175)。在比较不同药物类型联合美常安的效应均值时,观察到显著变异性的证据(P < 0.0001),并且发现柳氮磺胺吡啶在主要和次要结局方面都是最有效的药物。
有证据表明,美常安辅助治疗应被视为中国人群UC的标准治疗,因为它有助于诱导临床缓解,改善胃肠道症状并降低AE风险。