Drendel Amy L, Gray Matthew P, Lerner E Brooke
From the Departments of Pediatrics and.
Emergency Medicine and Pediatrics, Medical College of Wisconsin, Milwaukee, WI.
Pediatr Emerg Care. 2019 Jan;35(1):8-15. doi: 10.1097/PEC.0000000000001256.
Hospital trauma activation criteria are intended to identify children who are likely to require aggressive resuscitation or specific surgical interventions that are time sensitive and require the resources of a trauma team at the bedside. Evidence to support criteria is limited, and no prior publication has provided historical or current perspectives on hospital practices toward informing best practice. This study aimed to describe the published variation in (1) highest level of hospital trauma team activation criteria for pediatric patients and (2) hospital trauma team membership and (3) compare these finding to the current ACS recommendations.
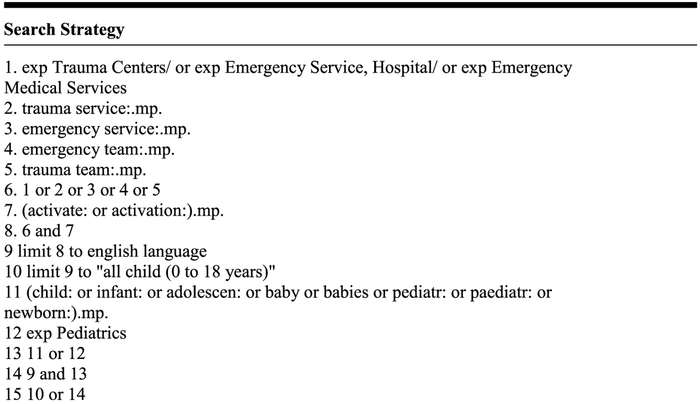
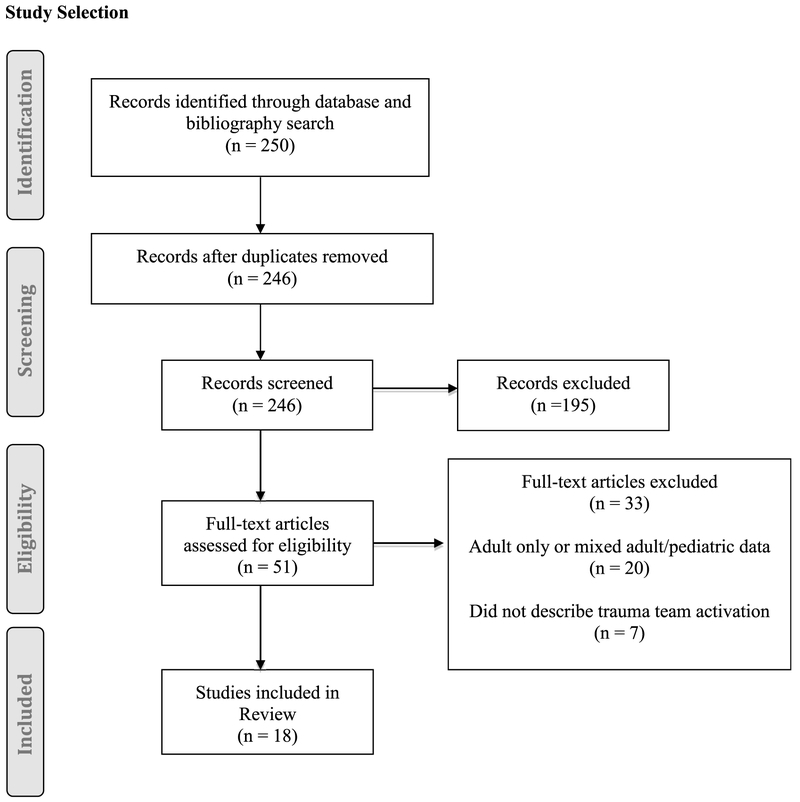
Using an Ovid MEDLINE In-Process & Other Non-Indexed Citations search, any published description of hospital trauma team activation criteria for children that used information captured in the prehospital setting was identified. Only studies of children were included. If the study included both adults and children, it was included if the number of children assessed with the criteria was included.
Eighteen studies spanning 20 years and 13,184 children were included. Hospital trauma team activation and trauma team membership were variable. Nearly all (92%) of the trauma criteria used physiologic factors. Penetrating trauma (83%) was frequently included in the trauma team activation criteria. Mechanisms of injury (52%) were least likely to be included in the highest level of activation. No predictable pattern of criterion adoption was found. Only 2 of the published criteria and 1 of published trauma team membership are consistent with the current American College of Surgeons recommendations.
Published hospital trauma team activation criteria and trauma team membership for children were variable. Future prospective studies are needed to define the optimal hospital trauma team activation criteria and trauma team membership and assess its impact on improving outcomes for children.
医院创伤启动标准旨在识别那些可能需要积极复苏或特定手术干预的儿童,这些干预对时间敏感,且需要床边创伤团队的资源。支持这些标准的证据有限,并且之前没有出版物提供关于医院实践以告知最佳实践的历史或当前观点。本研究旨在描述已发表的关于(1)儿科患者医院创伤团队启动标准的最高水平、(2)医院创伤团队成员构成的差异,并(3)将这些发现与美国外科医师学会(ACS)当前的建议进行比较。
通过Ovid MEDLINE在研及其他未索引引文搜索,识别出任何已发表的使用院前环境中获取信息的儿童医院创伤团队启动标准描述。仅纳入儿童研究。如果研究同时包括成人和儿童,若包含使用该标准评估的儿童数量,则纳入该研究。
纳入了跨越20年的18项研究,涉及13184名儿童。医院创伤团队启动和创伤团队成员构成各不相同。几乎所有(92%)的创伤标准都使用了生理因素。穿透性创伤(83%)经常被纳入创伤团队启动标准。损伤机制(52%)最不可能被纳入最高启动水平。未发现标准采用的可预测模式。已发表的标准中只有2项以及已发表的创伤团队成员构成中只有1项与美国外科医师学会当前的建议一致。
已发表的儿童医院创伤团队启动标准和创伤团队成员构成各不相同。未来需要进行前瞻性研究,以确定最佳的医院创伤团队启动标准和创伤团队成员构成,并评估其对改善儿童结局的影响。