Warwick Medical School, University of Warwick, Coventry, UK.
Worcester College, University of Oxford, Oxford, UK.
BMJ Open. 2019 Jan 23;9(1):e023687. doi: 10.1136/bmjopen-2018-023687.
We were commissioned by the behavioural insights team at Public Health England to synthesise the evidence on choice architecture interventions to increase healthy purchasing and/or consumption of food and drink by National Health Service (NHS) staff.
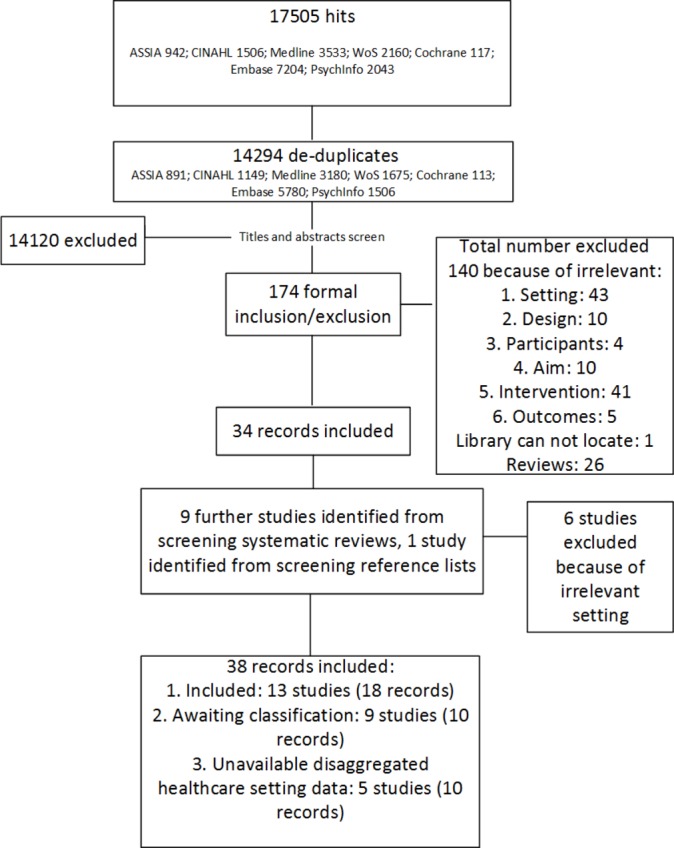
MEDLINE, EMBASE, CINAHL, Cochrane Central register of Controlled Trials, PsycINFO, Applied Social Sciences Index and Abstracts and Web of Science were searched from inception until May 2017 and references were screened independently by two reviewers.
A systematic review that included randomised experimental or intervention studies, interrupted time series and controlled before and after studies.
Healthcare staff of high-income countries.
Choice architecture interventions that aimed to improve dietary purchasing and/or consumption (outcomes) of staff.
Eligibility assessment, quality appraisal, data abstraction and analysis were completed by two reviewers. Quality appraisal of randomised trials was informed by the , and the Risk of Bias Assessment Tool for Nonrandomized Studies was used for the remainder. Findings were narratively synthesised.
Eighteen studies met the inclusion criteria. Five studies included multiple workplaces (including healthcare settings), 13 were conducted in healthcare settings only. Interventions in 10 studies were choice architecture only and 8 studies involved a complex intervention with a choice architecture element. Interventions involving a proximity element (making behavioural options easier or harder to engage with) appear to be frequently effective at changing behaviour. One study presented an effective sizing intervention. Labelling alone was generally not effective at changing purchasing behaviour. Interventions including an availability element were generally reported to be successful at changing behaviour but no included study examined this element alone. There was no strong evidence for the effect of pricing on purchasing or dietary intake.
Proximity, availability and sizing are choice architecture elements that are likely to be effective for NHS organisations.
CRD42017064872.
我们受英国公共卫生行为洞察团队委托,综合有关通过国家卫生服务(NHS)工作人员改变选择架构来增加健康食品和饮料购买和/或消费的证据。
从建库到 2017 年 5 月,我们在 MEDLINE、EMBASE、CINAHL、Cochrane 对照试验中心注册库、PsycINFO、应用社会科学索引和摘要以及 Web of Science 上进行了检索,并由两位评审员独立筛选参考文献。
系统综述,包括随机对照试验或干预研究、中断时间序列和对照前后研究。
高收入国家的医疗保健工作人员。
旨在改善工作人员饮食购买和/或消费(结果)的选择架构干预措施。
由两位评审员完成资格评估、质量评估、数据提取和分析。随机试验的质量评估依据了 ,其余的则采用非随机研究的偏倚风险评估工具。结果以叙述性方式进行综合。
符合纳入标准的有 18 项研究。5 项研究包括多个工作场所(包括医疗保健场所),13 项仅在医疗保健场所进行。10 项研究中的干预措施仅涉及选择架构,8 项研究涉及具有选择架构要素的复杂干预措施。涉及接近性要素(使行为选择更容易或更难参与)的干预措施似乎经常有效地改变行为。一项研究提出了一种有效的尺寸干预措施。仅标签通常不能有效改变购买行为。包括可用性要素的干预措施通常被报告为成功地改变了行为,但没有纳入的研究单独研究这一要素。没有强有力的证据表明价格对购买或饮食摄入有影响。
接近性、可用性和尺寸是 NHS 组织可能有效的选择架构要素。
CRD42017064872。