Bull World Health Organ. 1978;56(2):247-70.
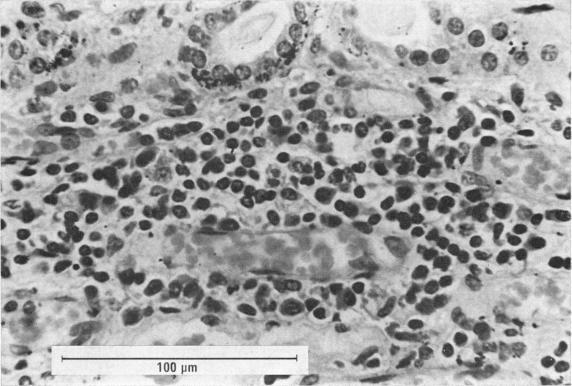
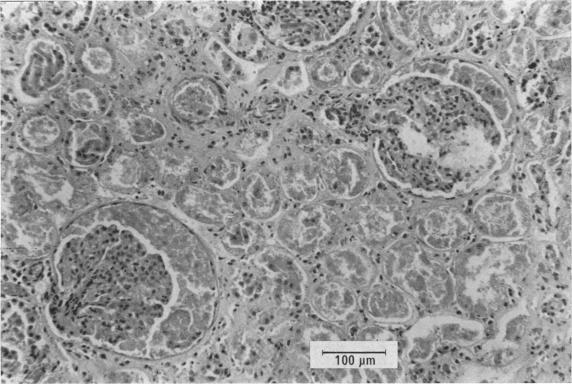
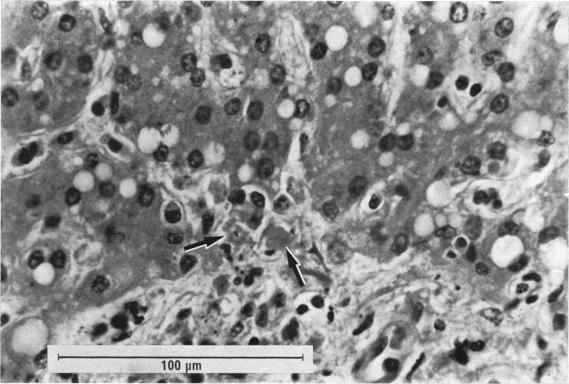
A large outbreak of haemorrhagic fever (subsequently named Ebola haemorrhagic fever) occurred in southern Sudan between June and November 1976. There was a total of 284 cases; 67 in the source town of Nzara, 213 in Maridi, 3 in Tembura, and 1 in Juba. The outbreak in Nzara appears to have originated in the workers of a cotton factory. The disease in Maridi was amplified by transmission in a large, active hospital. Transmission of the disease required close contact with an acute case and was usually associated with the act of nursing a patient. The incubation period was between 7 and 14 days. Although the link was not well established, it appears that Nzara could have been the source of infection for a similar outbreak in the Bumba Zone of Zaire.In this outbreak Ebola haemorrhagic fever was a unique clinical disease with a high mortality rate (53% overall) and a prolonged recovery period in those who survived. Beginning with an influenza-like syndrome, including fever, headache, and joint and muscle pains, the disease soon caused diarrhoea (81%), vomiting (59%), chest pain (83%), pain and dryness of the throat (63%), and rash (52%). Haemorrhagic manifestations were common (71%), being present in half of the recovered cases and in almost all the fatal cases.Two post mortems were carried out on patients in November 1976. The histopathological findings resembled those of an acute viral infection and although the features were characteristic they were not exclusively diagnostic. They closely resembled the features described in Marburg virus infection, with focal eosinophilic necrosis in the liver and destruction of lymphocytes and their replacement by plasma cells. One case had evidence of renal tubular necrosis.Two strains of Ebola virus were isolated from acute phase sera collected from acutely ill patients in Maridi hospital during the investigation in November 1976. Antibodies to Ebola virus were detected by immunofluorescence in 42 of 48 patients in Maridi who had been diagnosed clinically, but in only 6 of 31 patients in Nzara. The possibility of the indirect immunofluorescent test not being sufficiently sensitive is discussed.Of Maridi case contacts, in hospital and in the local community, 19% had antibodies. Very few of them gave any history of illness, indicating that Ebola virus can cause mild or even subclinical infections. Of the cloth room workers in the Nzara cotton factory, 37% appeared to have been infected, suggesting that the factory may have been the prime source of infection.
1976年6月至11月间,苏丹南部爆发了大规模出血热(后被命名为埃博拉出血热)。总共出现了284例病例;在源头城镇恩扎拉有67例,在马里迪有213例,在滕布拉有3例,在朱巴有1例。恩扎拉的疫情似乎起源于一家棉纺厂的工人。马里迪的疫情因在一家大型、活跃的医院内传播而加剧。该疾病的传播需要与急性期病例密切接触,且通常与护理患者的行为有关。潜伏期为7至14天。尽管联系并不十分明确,但恩扎拉似乎可能是扎伊尔邦布马区类似疫情的感染源。
在这次疫情中,埃博拉出血热是一种独特的临床疾病,死亡率很高(总体为53%),幸存者的恢复期也很长。疾病最初表现为类似流感的综合征,包括发热、头痛、关节和肌肉疼痛,很快就会引发腹泻(81%)、呕吐(59%)、胸痛(83%)、咽喉疼痛和干燥(63%)以及皮疹(52%)。出血表现很常见(71%),在半数康复病例和几乎所有死亡病例中都有出现。
1976年11月对两名患者进行了尸检。组织病理学检查结果类似于急性病毒感染,虽然这些特征具有一定特异性,但并非完全具有诊断性。它们与马尔堡病毒感染所描述的特征非常相似,肝脏出现局灶性嗜酸性坏死,淋巴细胞被破坏并被浆细胞取代。有一例有肾小管坏死的证据。
1976年11月调查期间,从马里迪医院急性病患者急性期血清中分离出两株埃博拉病毒。在马里迪临床诊断的48例患者中,有42例通过免疫荧光检测到埃博拉病毒抗体,但在恩扎拉的31例患者中只有6例检测到。文中讨论了间接免疫荧光试验可能不够灵敏的可能性。
在马里迪,医院和当地社区的病例接触者中,19%有抗体。他们中很少有人有患病史,这表明埃博拉病毒可引起轻度甚至亚临床感染。恩扎拉棉纺厂的布房工人中,37%似乎已被感染,这表明工厂可能是主要感染源。