Department of Oral Health Policy and Epidemiology, Harvard School of Dental Medicine, Boston, MA, USA.
Division of General Medicine and Clinical Epidemiology, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, NC, USA.
Med Decis Making. 2019 Apr;39(3):239-252. doi: 10.1177/0272989X19829735. Epub 2019 Feb 15.
Personalizing medical treatment often requires practitioners to compare multiple treatment options, assess a patient's unique risk and benefit from each option, and elicit a patient's preferences around treatment. We integrated these 3 considerations into a decision-modeling framework for the selection of second-line glycemic therapy for type 2 diabetes.
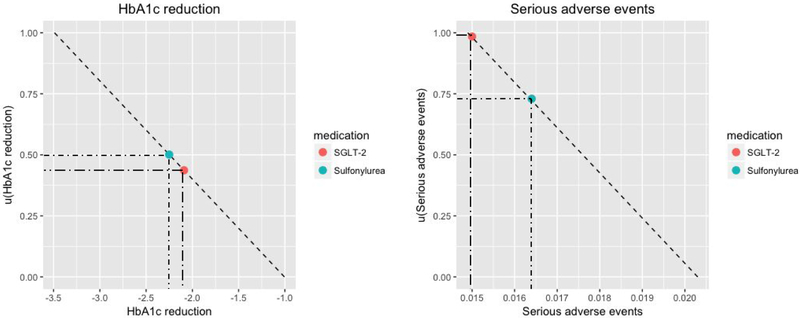
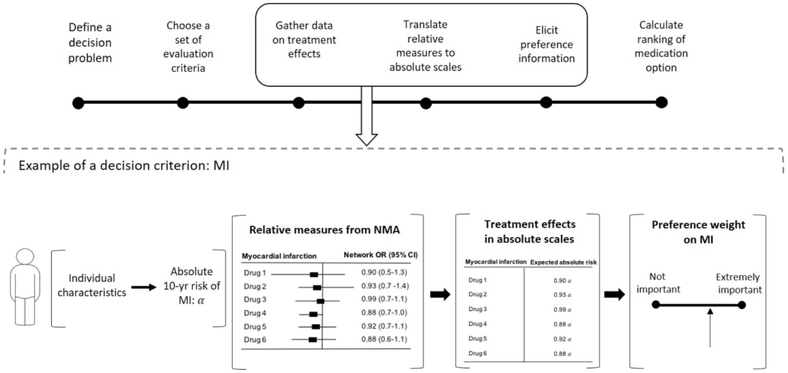
Based on multicriteria decision analysis, we developed a unified treatment decision support tool accounting for 3 factors: patient preferences, disease outcomes, and medication efficacy and safety profiles. By standardizing and multiplying these 3 factors, we calculated the ranking score for each medication. This approach was applied to determining second-line glycemic therapy by integrating 1) treatment efficacy and side-effect data from a network meta-analysis of 301 randomized trials ( N = 219,277), 2) validated risk equations for type 2 diabetes complications, and 3) patient preferences around treatment (e.g., to avoid daily glucose testing). Data from participants with type 2 diabetes in the U.S. National Health and Nutrition Examination Survey (NHANES 2003-2014, N = 1107) were used to explore variations in treatment recommendations and associated quality-adjusted life-years given different patient features.
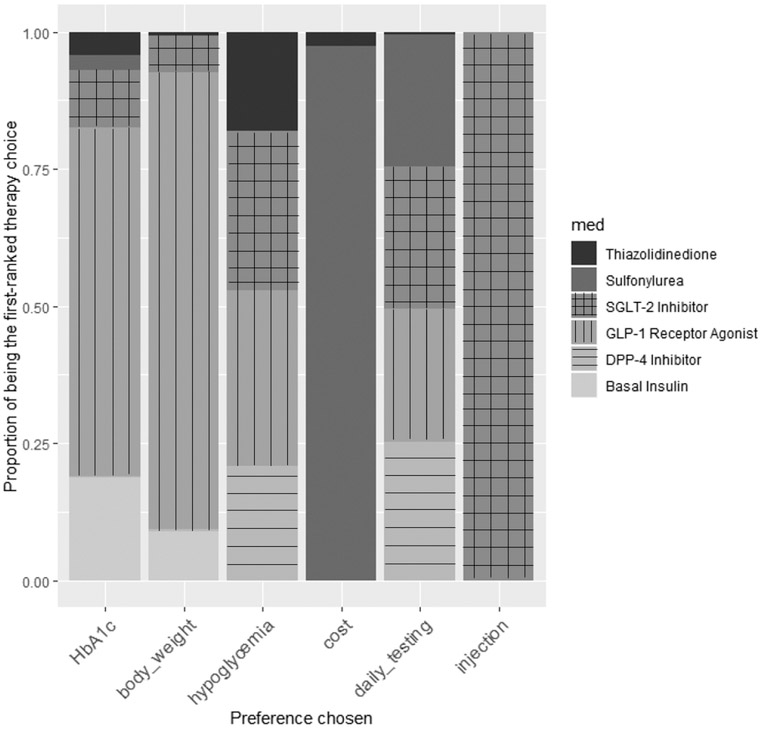
Patients at the highest microvascular disease risk had glucagon-like peptide 1 agonists or basal insulin recommended as top choices, whereas those wanting to avoid an injected medication or daily glucose testing had sodium-glucose linked transporter 2 or dipeptidyl peptidase 4 inhibitors commonly recommended, and those with major cost concerns had sulfonylureas commonly recommended. By converting from the most common sulfonylurea treatment to the model-recommended treatment, NHANES participants were expected to save an average of 0.036 quality-adjusted life-years per person (about a half month) from 10 years of treatment.
Models can help integrate meta-analytic treatment effect estimates with individualized risk calculations and preferences, to aid personalized treatment selection.
为患者制定个性化治疗方案通常需要临床医生比较多种治疗方案,评估患者从每种方案中获得的独特风险和获益,并了解患者对治疗方案的偏好。我们将这 3 个方面整合到一个决策模型框架中,用于选择 2 型糖尿病的二线血糖治疗方案。
基于多准则决策分析,我们开发了一个统一的治疗决策支持工具,考虑了 3 个因素:患者偏好、疾病结局和药物疗效及安全性特征。通过对这 3 个因素进行标准化和相乘,我们计算了每种药物的排名得分。该方法应用于通过整合以下 3 个方面来确定二线血糖治疗方案:1)来自 301 项随机试验的网络荟萃分析(N=219277)的治疗效果和副作用数据;2)验证的 2 型糖尿病并发症风险方程;3)患者对治疗的偏好(例如,避免每日血糖检测)。使用来自美国国家健康和营养调查(NHANES 2003-2014,N=1107)的 2 型糖尿病患者的数据,探讨了不同患者特征下的治疗推荐和相关质量调整生命年的变化。
微血管疾病风险最高的患者推荐使用胰高血糖素样肽 1 激动剂或基础胰岛素作为首选,而那些希望避免注射药物或每日血糖检测的患者则推荐使用钠-葡萄糖协同转运蛋白 2 或二肽基肽酶 4 抑制剂,那些主要关注成本的患者则推荐使用磺酰脲类药物。将最常见的磺酰脲类药物治疗转换为模型推荐的治疗方案,NHANES 参与者预计将从 10 年的治疗中平均每人节省 0.036 个质量调整生命年(约半个月)。
模型可以帮助整合荟萃分析的治疗效果估计与个体化风险计算和偏好,以辅助个性化治疗选择。