Anaesthesiology and Critical Care, Hospital de León, University Hospital Complex, C/Altos de Nava s/n, 24071, Leon, Spain.
J Clin Monit Comput. 2020 Feb;34(1):89-95. doi: 10.1007/s10877-019-00285-0. Epub 2019 Feb 19.
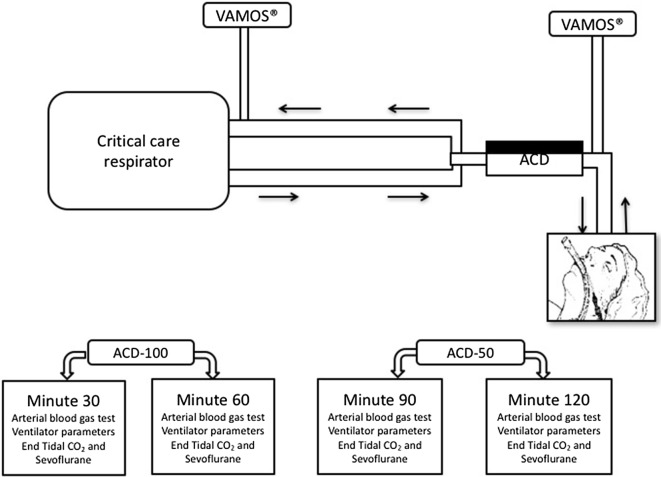
Changes have been made to the AnaConDa device (Sedana Medical, Stockholm, Sweden), decreasing its size to reduce dead space and carbon dioxide (CO) retention. However, this also involves a decrease in the surface area of the activated carbon filter. The CO elimination and sevoflurane (SEV) reflection of the old device (ACD-100) were thus compared with the new version (ACD-50) in patients sedated after coronary artery bypass graft surgery. After ERC approval and written informed consent, 23 patients were sedated with SEV, using first the ACD-100 and then the ACD-50 for 60 min each. With each device, patients were ventilated with tidal volumes (TV) of 5 ml/kg of ideal body weight for the first 30 min, and with 7 ml/kg for the next 30 min. Ventilation parameters, arterial blood gases, Bispectral-Index™ (BIS, Aspect Medical Systems Inc., Newton, MA, USA), SEV concentrations exhaled by the patient (SEV-exhaled) and from the expiratory hose (SEV-lost) were recorded every 30 min. A SEV reflection index was calculated: SRI [%] = 100 × (1 - (SEV-lost/SEV-exhaled)). Data were compared using ANOVA with repeated measurements and Student's T-tests for pairs. Respiratory rates, tidal and minute volumes were not significantly different between the two devices. End tidal and arterial CO partial pressures were significantly higher with the ACD-100 as compared with the ACD-50. SEV infusion rate remained constant. SEV reflection was higher (SRI: ACD-100 vs. ACD-50, TV 5 ml/kg: 95.29 ± 6.45 vs. 85.54 ± 11.15, p = 0.001; 7 ml/kg: 93.42 ± 6.55 vs. 88.77 ± 12.26, p = 0.003). BIS was significantly lower when using the higher TV (60.91 ± 9.99 vs. 66.57 ± 8.22, p = 0.012), although this difference was not clinically relevant. During postoperative sedation, the use of ACD-50 significantly reduced CO retention. SEV reflection was slightly reduced. However, patients remained sufficiently sedated without increasing SEV infusion.
AnaConDa 仪器(Sedana Medical,斯德哥尔摩,瑞典)的尺寸有所减小,以减少死腔和二氧化碳(CO)潴留。然而,这也会导致活性炭过滤器的表面积减小。因此,在冠状动脉旁路移植手术后接受镇静的患者中,比较了旧版设备(ACD-100)和新版设备(ACD-50)的 CO 清除率和七氟醚(SEV)反射率。经过 ERC 批准和书面知情同意,23 名患者使用 SEV 镇静,先使用 ACD-100 镇静 60 分钟,然后使用 ACD-50 镇静 60 分钟。在每个设备中,患者在前 30 分钟内以理想体重 5ml/kg 的潮气量(TV)通气,在接下来的 30 分钟内以 7ml/kg 的 TV 通气。每 30 分钟记录一次通气参数、动脉血气、BIS(Aspect Medical Systems Inc.,牛顿,MA,美国)、患者呼出的 SEV 浓度(SEV-exhaled)和呼气软管中的 SEV 浓度(SEV-lost)。计算 SEV 反射指数:SRI [%] = 100 × (1 - (SEV-lost/SEV-exhaled))。使用重复测量方差分析和学生 T 检验进行成对比较。两种设备之间的呼吸频率、潮气量和分钟通气量无显著差异。与 ACD-50 相比,ACD-100 的呼气末和动脉 CO 分压显著升高。SEV 输注率保持不变。SEV 反射率较高(SRI:ACD-100 与 ACD-50,TV 5ml/kg:95.29 ± 6.45 与 85.54 ± 11.15,p = 0.001;7ml/kg:93.42 ± 6.55 与 88.77 ± 12.26,p = 0.003)。使用较高 TV 时,BIS 显著降低(60.91 ± 9.99 与 66.57 ± 8.22,p = 0.012),尽管这种差异无临床意义。在术后镇静期间,使用 ACD-50 可显著减少 CO 潴留。SEV 反射率略有降低。然而,患者仍然保持足够的镇静状态,而无需增加 SEV 输注。