Department of Neurology, Neuro ICU, Groupe Hospitalier Pitié-Salpêtrière, AP-HP, Paris, France.
Institut du Cerveau et de la Moelle épinière, ICM, PICNIC lab, F-75013, Paris, France.
BMJ Open. 2019 Feb 21;9(2):e026211. doi: 10.1136/bmjopen-2018-026211.
The clinical distinction between vegetative state/unresponsive wakefulness syndrome (UWS) and minimally conscious state (MCS) is a key step to elaborate a prognosis and formulate an appropriate medical plan for any patient suffering from disorders of consciousness (DoC). However, this assessment is often challenging and may require specialised expertise. In this study, we hypothesised that pooling subjective reports of the level of consciousness of a given patient across several nursing staff members can be used to clinically detect MCS.
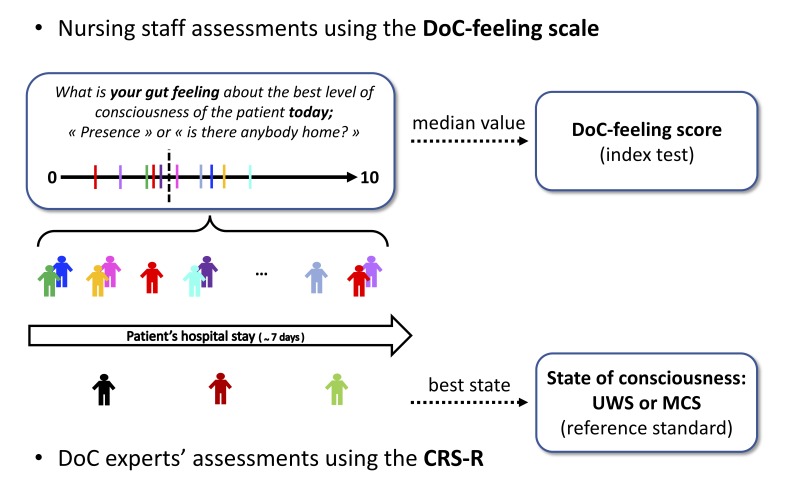
Patients referred to consciousness assessment were prospectively screened. MCS (target condition) was defined according to the best Coma Recovery Scale-Revised score (CRS-R) obtained from expert physicians (reference standard). 'DoC-feeling' score was defined as the median of individual subjective reports pooled from multiple staff members during a week of hospitalisation (index test). Individual ratings were collected at the end of each shift using a 100 mm Visual Analogue Scale, blinded from the reference standard. Diagnostic accuracy was evaluated using area under the receiver operating characteristic curve (AUC), sensitivity and specificity metrics.
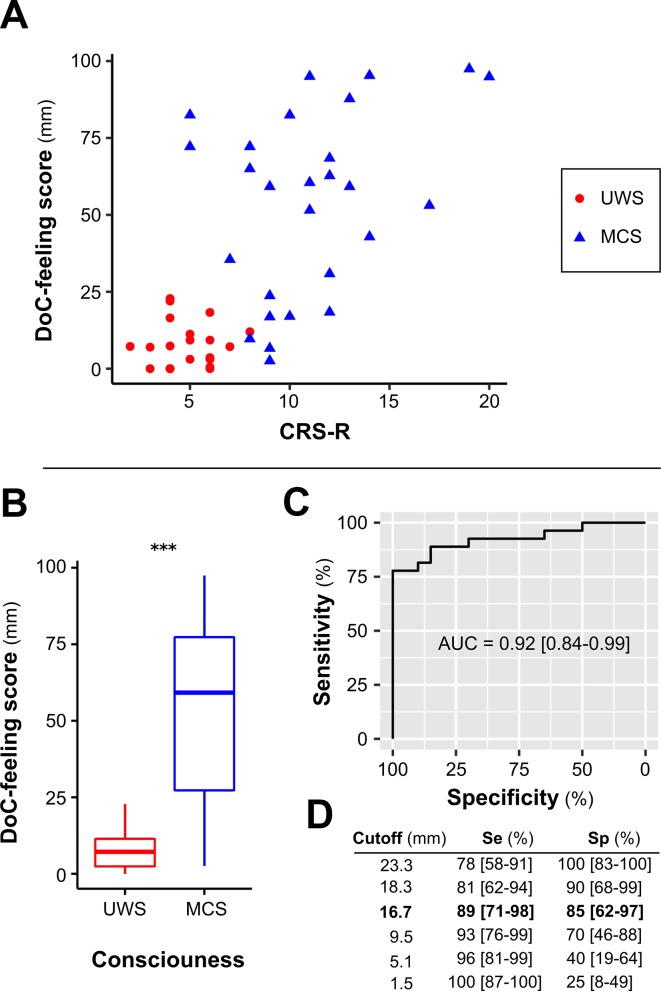
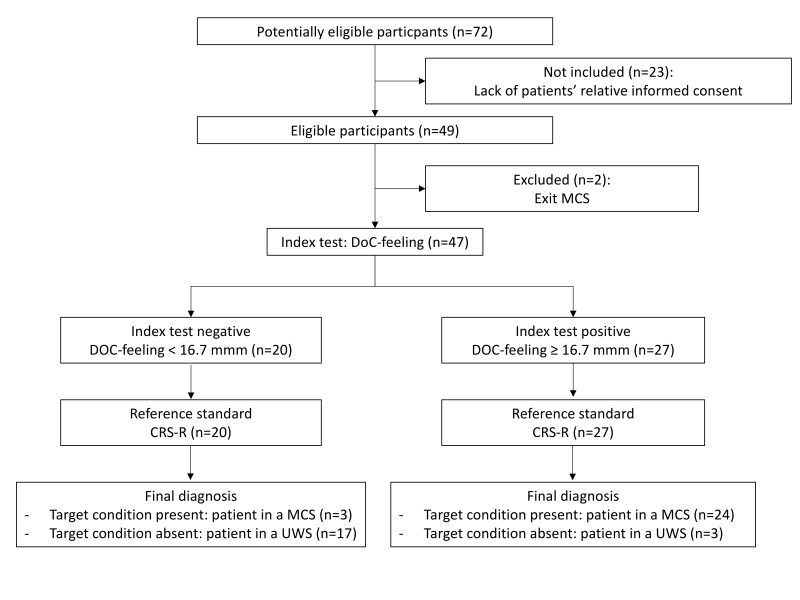
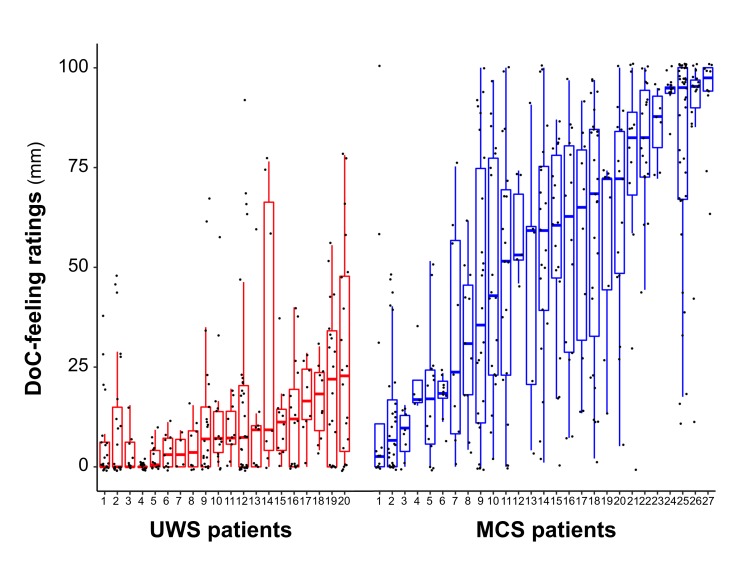
692 ratings performed by 83 nursing staff members were collected from 47 patients. Twenty patients were diagnosed with UWS and 27 with MCS. DoC-feeling scores obtained by pooling all individual ratings obtained for a given patient were significantly greater in patients with MCS than with UWS (59.2 mm (IQR: 27.3-77.3) vs 7.2 mm (IQR: 2.4-11.4); p<0.001) yielding an AUC of 0.92 (95% CI 0.84 to 0.99).
DoC-feeling capitalises on the expertise of nursing staff to evaluate patients' consciousness. Together with the CRS-R as well as with brain imaging, DoC-feeling might improve diagnostic and prognostic accuracy of patients with DoC.
植物状态/无反应性觉醒综合征(UWS)和最小意识状态(MCS)的临床鉴别是为任何患有意识障碍(DoC)的患者制定预后和制定适当医疗计划的关键步骤。然而,这种评估通常具有挑战性,可能需要专门的专业知识。在这项研究中,我们假设可以通过汇集多名护理人员对给定患者意识水平的主观报告,用于临床检测 MCS。
前瞻性筛选了接受意识评估的患者。MCS(目标条件)根据专家医生获得的最佳昏迷恢复量表修订版(CRS-R)得分(参考标准)定义。“DoC 感觉”评分定义为住院期间一周内从多名工作人员汇总的个体主观报告的中位数(索引测试)。使用 100mm 视觉模拟量表在每个班次结束时进行个体评分,该量表与参考标准相盲。使用接受者操作特征曲线(ROC)下面积(AUC)、敏感性和特异性指标评估诊断准确性。
从 47 名患者中收集了 83 名护理人员进行的 692 次评分。20 名患者被诊断为 UWS,27 名患者被诊断为 MCS。通过汇集给定患者的所有个体评分获得的 DoC 感觉评分在 MCS 患者中明显高于 UWS 患者(59.2mm(IQR:27.3-77.3)与 7.2mm(IQR:2.4-11.4);p<0.001),AUC 为 0.92(95%CI 0.84-0.99)。
DoC 感觉利用护理人员的专业知识来评估患者的意识。与 CRS-R 以及脑成像一起,DoC 感觉可能会提高 DoC 患者的诊断和预后准确性。