Department of Cancer Physiology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA; Institute of Biomedical Engineering, Bogazici University, Istanbul, Turkey.
Department of Thoracic Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA.
Lung Cancer. 2019 Mar;129:75-79. doi: 10.1016/j.lungcan.2019.01.010. Epub 2019 Jan 23.
Immune-checkpoint blockades have exhibited durable responses and improved long-term survival in a subset of advanced non-small cell lung cancer (NSCLC) patients. However, highly predictive markers of positive and negative responses to immunotherapy are a significant unmet clinical need. The objective of this study was to identify clinical and computational image-based predictors of rapid disease progression phenotypes in NSCLC patients treated with immune-checkpoint blockades.
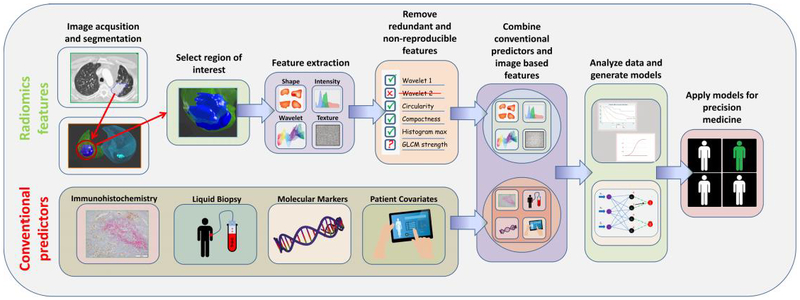
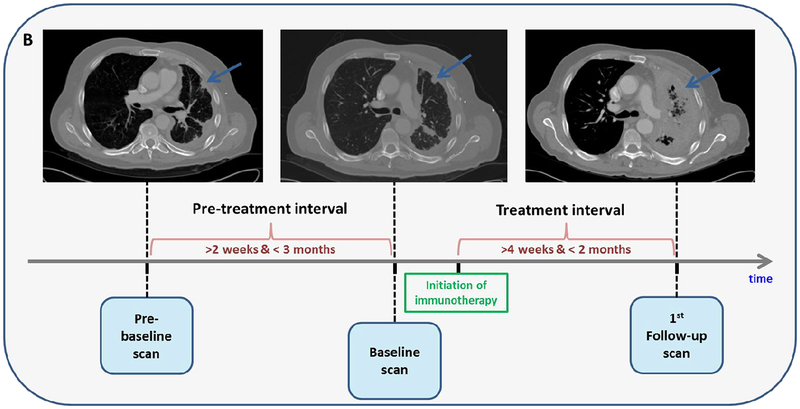
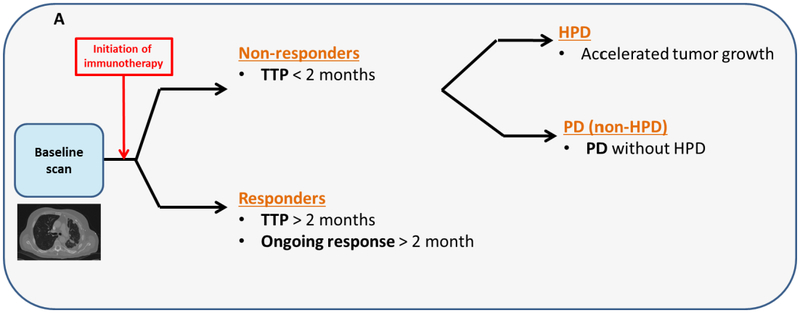
Using time-to-progression (TTP) and/or tumor growth rates, rapid disease progression phenotypes were developed including hyperprogressive disease. The pre-treatment baseline predictors that were used to identify these phenotypes included patient demographics, clinical data, driver mutations, hematology data, and computational image-based features (radiomics) that were extracted from pre-treatment computed tomography scans. Synthetic Minority Oversampling Technique (SMOTE) was used to subsample minority groups to eliminate classification bias. Patient-level probabilities were calculated from the final clinical-radiomic models to subgroup patients by progression-free survival (PFS).
Among 228 NSCLC patients treated with single agent or double agent immunotherapy, we identified parsimonious clinical-radiomic models with modest to high ability to predict rapid disease progression phenotypes with area under the receiver-operator characteristics ranging from 0.804 to 0.865. Patients who had TTP < 2 months or hyperprogressive disease were classified with 73.41% and 82.28% accuracy after SMOTE subsampling, respectively. When the patient subgroups based on patient-level probabilities were analyzed for survival outcomes, patients with higher probability scores had significantly worse PFS.
The models found in this study have potential important translational implications to identify highly vulnerable NSCLC patients treated with immunotherapy that experience rapid disease progression and poor survival outcomes.
免疫检查点阻断在一部分晚期非小细胞肺癌(NSCLC)患者中显示出持久的反应和改善的长期生存。然而,免疫治疗阳性和阴性反应的高度预测标志物是一个重大的未满足的临床需求。本研究的目的是确定接受免疫检查点阻断治疗的 NSCLC 患者中快速疾病进展表型的临床和计算影像学预测因子。
使用无进展生存期(PFS)和/或肿瘤生长率,开发了快速疾病进展表型,包括超进展性疾病。用于识别这些表型的基线预测因子包括患者人口统计学、临床数据、驱动突变、血液学数据和从治疗前 CT 扫描提取的计算影像学特征(放射组学)。合成少数过采样技术(SMOTE)用于对少数群体进行亚采样,以消除分类偏差。从最终的临床放射组学模型中计算患者水平的概率,以根据无进展生存期(PFS)对患者进行亚组分组。
在 228 名接受单药或双药免疫治疗的 NSCLC 患者中,我们确定了具有适度至高度预测快速疾病进展表型能力的简约临床放射组学模型,其接受者操作特征曲线下面积(AUC)范围为 0.804 至 0.865。经过 SMOTE 亚采样后,无进展生存期(PFS)分别为 73.41%和 82.28%,将 TTP<2 个月或超进展性疾病的患者分类。当根据患者水平概率对生存结果进行亚组分析时,具有较高概率评分的患者的 PFS 明显更差。
本研究中发现的模型具有潜在的重要转化意义,可以识别接受免疫治疗后快速疾病进展和生存结局较差的高危 NSCLC 患者。