Taneja Charu, Netsch Debra, Rolstad Bonnie Sue, Inglese Gary, Eaves Deanna, Oster Gerry
Charu Taneja, MPH, Policy Analysis Inc (PAI), Brookline, Massachusetts. Debra Netsch, DNP, APRN, CNP, CWOCN, webWOC Nursing Education Program, Minneapolis, Minnesota. Bonnie Sue Rolstad, MS, RN, CWOCN, webWOC Education Programs, Metropolitan State University, Minneapolis, Minnesota. Gary Inglese, MBA, RN, Hollister Incorporated, Libertyville, Illinois. Deanna Eaves, BS, Hollister Incorporated, Libertyville, Illinois. Gerry Oster, PhD, Policy Analysis Inc (PAI), Brookline, Massachusetts.
J Wound Ostomy Continence Nurs. 2019 Mar/Apr;46(2):143-149. doi: 10.1097/WON.0000000000000509.
The purpose of this study was to examine the incidence and economic burden of peristomal skin complications (PSCs) following ostomy surgery.
Retrospective cohort study based on electronic health records and administrative data stores at a large US integrated healthcare system.
The sample comprised 168 patients who underwent colostomy (ICD-9-CM 46.1X) (n = 108), ileostomy (46.2X) (n = 40), cutaneous ureteroileostomy (56.5X), or other external urinary diversion (56.6X) (n = 20) between January 1, 2012, and December 31, 2014. The study setting was an integrated health services organization that serves more than 2 million persons in the northeastern United States.
We scanned electronic health records of all study subjects to identify those with evidence of PSCs within 90 days of ostomy surgery and then examined healthcare utilization and costs over 120 days, beginning with date of surgery, among patients with and without evidence of PSCs. Testing for differences in continuous measures between the 3 ostomy groups was based on one-way analysis of variance; testing for differences in such measures between the PSC and non-PSC groups was based on a t statistic, and the χ statistic was used to test for differences in categorical measures.
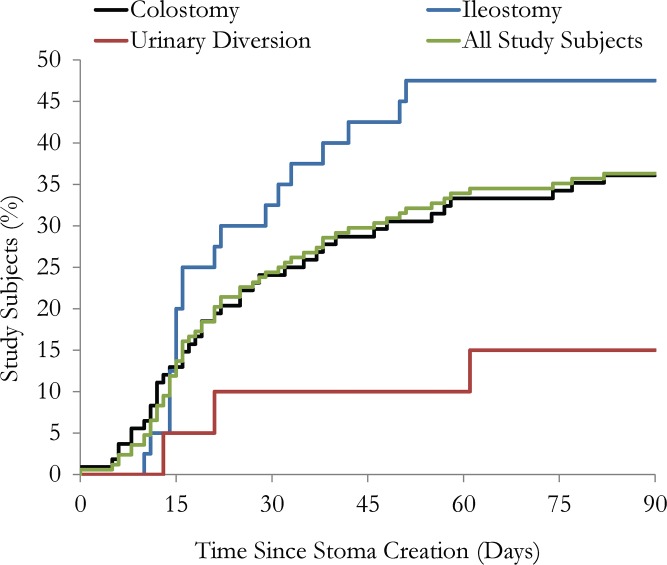
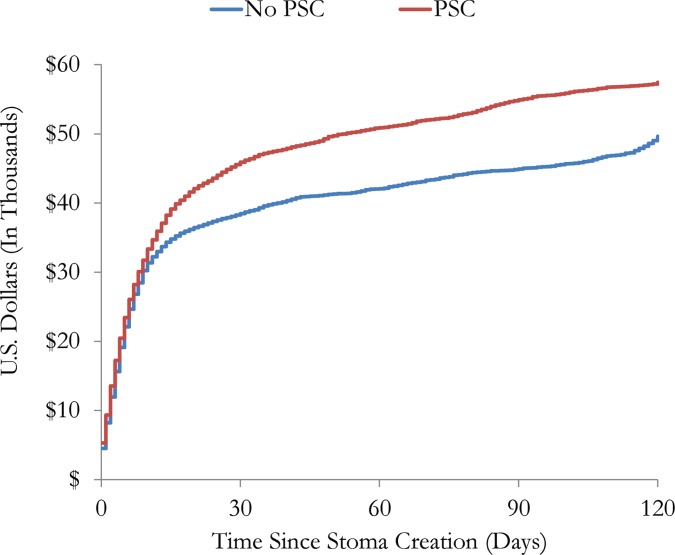
Sixty-one subjects (36.3%) had evidence of PSCs within 90 days of ostomy surgery (ileostomy, 47.5%; colostomy, 36.1%; urinary diversion, 15.0%; P < .05 for differences between groups). Among patients with evidence of PSCs, the mean (SD) time from surgery to first notation of this complication was 26.4 (19.0) days; it was 24.1 (13.2) days for ileostomy, 27.2 (21.1) days for colostomy, and 31.7 (25.7) days for urinary diversion (P = .752). Patients with PSCs were more likely to be readmitted to hospital by day 120 (55.7% vs 35.5% for those without PSCs; P = .011). The mean length of stay for patients readmitted to hospital was 11.0 days for those with PSCs and 6.8 days for those without PSCs (P = .111). The mean total healthcare cost over 120 days was $58,329 for patients with evidence of PSCs and $50,298 for those without evidence of PSCs (P = .251).
Approximately one-third of ostomy patients developed PSCs within 90 days of their surgery. Peristomal skin complications are associated with a greater likelihood of hospital readmission. Our findings corroborate results of earlier studies.
本研究旨在调查造口术后造口周围皮肤并发症(PSC)的发生率及经济负担。
基于美国一个大型综合医疗系统的电子健康记录和管理数据存储进行的回顾性队列研究。
样本包括2012年1月1日至2014年12月31日期间接受结肠造口术(国际疾病分类第九版临床修订本[ICD-9-CM]编码46.1X)(n = 108)、回肠造口术(46.2X)(n = 40)、皮肤输尿管回肠造口术(56.5X)或其他外部尿路改道术(56.6X)(n = 20)的168例患者。研究背景为一个为美国东北部200多万人提供服务的综合健康服务机构。
我们扫描了所有研究对象的电子健康记录,以识别造口术后90天内有PSC证据的患者,然后从手术日期开始,检查有和没有PSC证据的患者在120天内的医疗服务利用情况和费用。对3个造口组之间连续指标差异的检验基于单因素方差分析;对PSC组和非PSC组之间此类指标差异的检验基于t统计量,χ统计量用于检验分类指标的差异。
61例患者(36.3%)在造口术后90天内有PSC证据(回肠造口术,47.5%;结肠造口术,36.1%;尿路改道术,15.0%;组间差异P <.05)。在有PSC证据的患者中,从手术到首次记录该并发症的平均(标准差)时间为26.4(19.0)天;回肠造口术为24.1(13.2)天,结肠造口术为27.2(21.1)天,尿路改道术为31.7(25.7)天(P =.752)。有PSC的患者在120天内再次入院的可能性更大(55.7%对无PSC者的35.5%;P =.011)。再次入院患者的平均住院时间,有PSC的患者为11.0天,无PSC的患者为6.8天(P =.111)。有PSC证据的患者在120天内的平均总医疗费用为58,329美元,无PSC证据的患者为50,298美元(P =.251)。
约三分之一的造口患者在术后90天内发生PSC。造口周围皮肤并发症与再次入院的可能性更大有关。我们的研究结果证实了早期研究的结果。