Alansary Amin Mohammed, Elbeialy Marwa Ahmed Khairy
Department of Anesthesiology, Intensive Care and Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt.
Saudi J Anaesth. 2019 Apr-Jun;13(2):119-125. doi: 10.4103/sja.SJA_600_18.
The literature on drugs used for combined general anesthesia and epidural analgesia (CGE) in lumbar operations is scarce. The purpose of the study was to compare the addition of either dexmedetomidine or fentanyl to bupivacaine for epidural analgesia in combination with general anesthesia with regard to efficacy and adverse events in such operations.
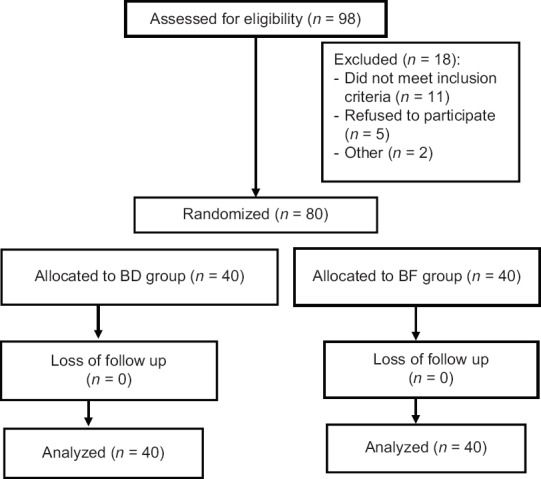
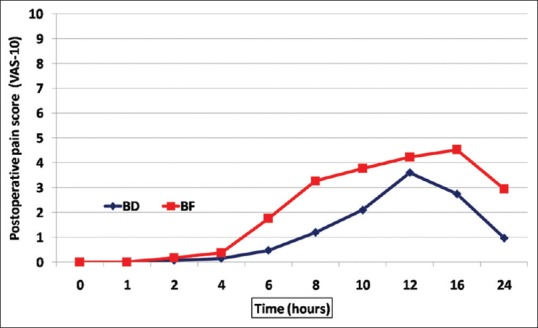
This prospective, randomized, double-blinded study was conducted on 80 patients who were scheduled for an elective lumbar disc operation, age 20-65 years, of either sex and American Society of Anesthesiologists physical status I or II. They were randomly allocated into one of the two groups - group bupivacaine-dexmedetomidine (BD) ( = 40): patients who received CGE with 15 mL of bupivacaine 0.20% plus 50 μg of dexmedetomidine and group bupivacaine-fentanyl (BF) ( = 40): patients who received CGE with 15 mL of bupivacaine 0.20% plus 50 μg fentanyl. The primary outcome was time to first analgesic requirement, whereas the secondary outcomes were the total opioid consumption and pain scores during the first 24 h. The incidence of adverse postoperative (PO) effects related to the study drugs, such as sedation, nausea and vomiting, pruritus, shivering, and respiratory depression, was also documented.
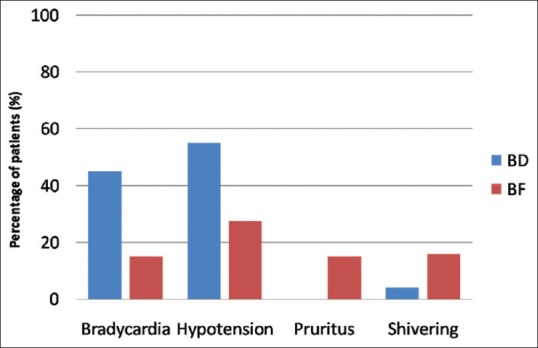
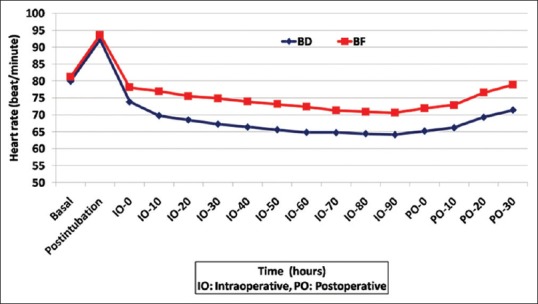
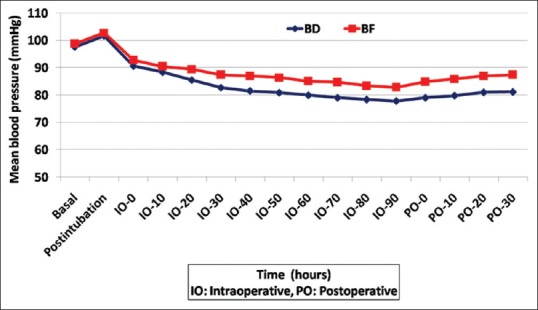
Patients in the BD group experienced a significantly prolonged pain-free period, lower total opioid consumption, and lower pain scores than patients in the BF group ( < 0.001). Patients in the BD group showed a significantly lower intraoperative heart rate and mean blood pressure ( < 0.001). Regarding adverse events, there were greater PO sedation scores ( < 0.001) and less frequent episodes of PO nausea and vomiting in the BD group. In addition, patients in the BD group showed less pruritis and shivering. There were no reported cases of respiratory depression in either group.
CGE with bupivacaine plus dexmedetomidine provided better PO pain control than bupivacaine plus fentanyl, with fewer adverse events overall.
关于用于腰椎手术的全身麻醉联合硬膜外镇痛(CGE)的药物的文献较少。本研究的目的是比较在全身麻醉联合硬膜外镇痛中,将右美托咪定或芬太尼添加到布比卡因中用于硬膜外镇痛的疗效和不良事件。
本前瞻性、随机、双盲研究纳入了80例计划进行择期腰椎间盘手术的患者,年龄20 - 65岁,性别不限,美国麻醉医师协会身体状况分级为I或II级。他们被随机分为两组之一——布比卡因 - 右美托咪定组(BD组)(n = 40):接受15 mL 0.20%布比卡因加50 μg右美托咪定进行CGE的患者;布比卡因 - 芬太尼组(BF组)(n = 40):接受15 mL 0.20%布比卡因加50 μg芬太尼进行CGE的患者。主要结局是首次需要镇痛的时间,次要结局是前24小时内的总阿片类药物消耗量和疼痛评分。还记录了与研究药物相关的术后不良事件的发生率,如镇静、恶心和呕吐、瘙痒、寒战和呼吸抑制。
与BF组患者相比,BD组患者的无痛期显著延长,总阿片类药物消耗量更低,疼痛评分更低(P < 0.001)。BD组患者术中心率和平均血压显著更低(P < 0.001)。关于不良事件,BD组术后镇静评分更高(P < 0.001),术后恶心和呕吐发作频率更低。此外,BD组患者瘙痒和寒战更少。两组均未报告呼吸抑制病例。
布比卡因加右美托咪定的CGE比布比卡因加芬太尼提供了更好的术后疼痛控制,总体不良事件更少。