Harvard T H Chan School of Public Health, Harvard University, Boston, MA, USA.
Institute for Health Metrics and Evaluation, University of Washington, Seattle, WA, USA.
Lancet HIV. 2019 Jun;6(6):e382-e395. doi: 10.1016/S2352-3018(19)30038-4. Epub 2019 Apr 26.
Between 2012 and 2016, development assistance for HIV/AIDS decreased by 20·0%; domestic financing is therefore critical to sustaining the response to HIV/AIDS. To understand whether domestic resources could fill the financing gaps created by declines in development assistance, we aimed to track spending on HIV/AIDS and estimated the potential for governments to devote additional domestic funds to HIV/AIDS.
We extracted 8589 datapoints reporting spending on HIV/AIDS. We used spatiotemporal Gaussian process regression to estimate a complete time series of spending by domestic sources (government, prepaid private, and out-of-pocket) and spending category (prevention, and care and treatment) from 2000 to 2016 for 137 low-income and middle-income countries (LMICs). Development assistance data for HIV/AIDS were from Financing Global Health 2018, and HIV/AIDS prevalence, incidence, and mortality were from the Global Burden of Disease study 2017. We used stochastic frontier analysis to estimate potential additional government spending on HIV/AIDS, which was conditional on the current government health budget and other finance, economic, and contextual factors associated with HIV/AIDS spending. All spending estimates were reported in 2018 US$.
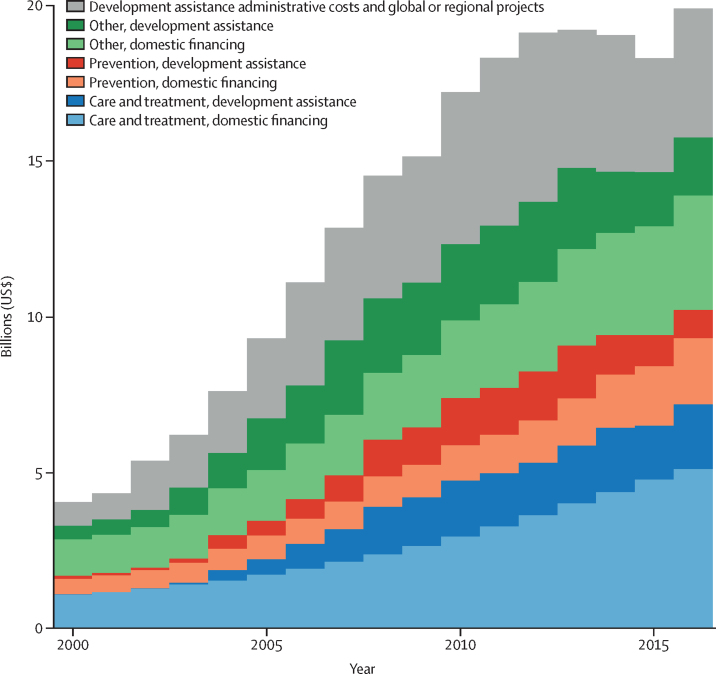
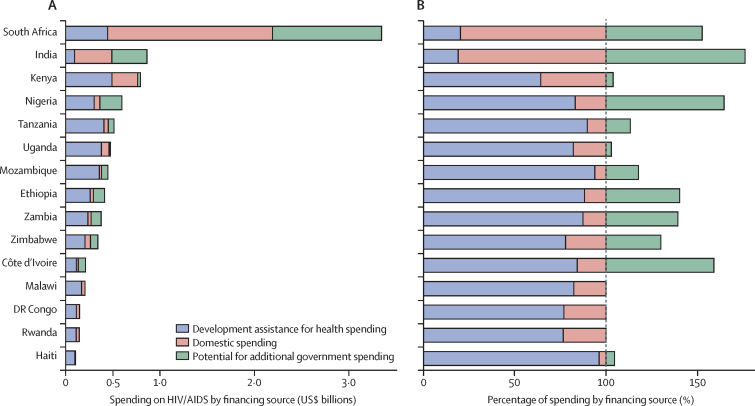
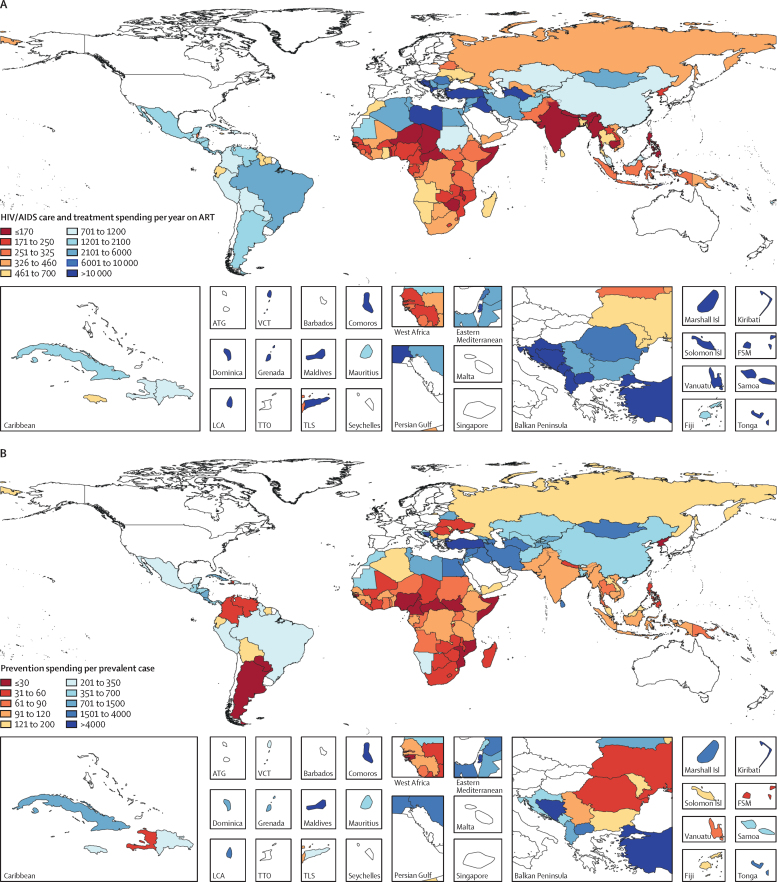
Between 2000 and 2016, total spending on HIV/AIDS in LMICs increased from $4·0 billion (95% uncertainty interval 2·9-6·0) to $19·9 billion (15·8-26·3), spending on HIV/AIDS prevention increased from $596 million (258 million to 1·3 billion) to $3·0 billion (1·5-5·8), and spending on HIV/AIDS care and treatment increased from $1·1 billion (458·1 million to 2·2 billion) to $7·2 billion (4·3-11·8). Over this time period, the share of resources sourced from development assistance increased from 33·2% (21·3-45·0) to 46·0% (34·2-57·0). Care and treatment spending per year on antiretroviral therapy varied across countries, with an IQR of $284-2915. An additional $12·1 billion (8·4-17·5) globally could be mobilised by governments of LMICs to finance the response to HIV/AIDS. Most of these potential resources are concentrated in ten middle-income countries (Argentina, China, Colombia, India, Indonesia, Mexico, Nigeria, Russia, South Africa, and Vietnam).
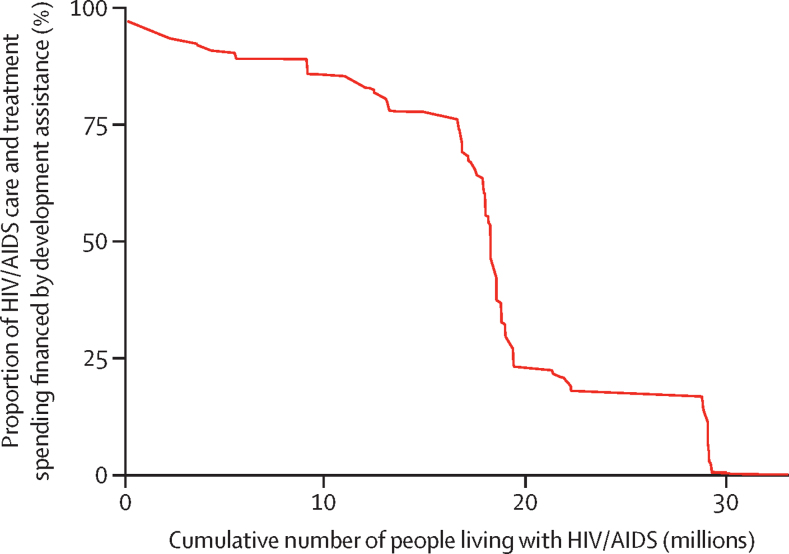
Some governments could mobilise more domestic resources to fight HIV/AIDS, which could free up additional development assistance for many countries without this ability, including many low-income, high-prevalence countries. However, a large gap exists between available financing and the funding needed to achieve global HIV/AIDS goals, and sustained and coordinated effort across international and domestic development partners is required to end AIDS by 2030.
The Bill & Melinda Gates Foundation.
2012 年至 2016 年期间,艾滋病毒/艾滋病防治的发展援助减少了 20.0%;因此,国内供资对于维持对艾滋病毒/艾滋病的应对至关重要。为了了解国内资源是否能够填补发展援助减少造成的资金缺口,我们旨在跟踪艾滋病毒/艾滋病支出情况,并评估各国将更多国内资金用于艾滋病毒/艾滋病的潜力。
我们提取了 8589 个数据点,报告了艾滋病毒/艾滋病支出情况。我们使用时空高斯过程回归,从 2000 年到 2016 年,对 137 个低收入和中等收入国家(LMICs)的国内来源(政府、预付款私人和自付)和支出类别(预防和护理与治疗)的完整时间序列进行了估计。艾滋病毒/艾滋病发展援助数据来自 2018 年全球卫生融资,艾滋病毒/艾滋病流行率、发病率和死亡率来自 2017 年全球疾病负担研究。我们使用随机前沿分析来估计艾滋病毒/艾滋病方面的潜在额外政府支出,这取决于当前的政府卫生预算和与艾滋病毒/艾滋病支出相关的其他财政、经济和背景因素。所有支出估计均以 2018 年的美元报告。
2000 年至 2016 年间,LMICs 的艾滋病毒/艾滋病总支出从 40 亿美元(95%置信区间 29 亿至 60 亿美元)增加到 199 亿美元(158 亿至 263 亿美元),艾滋病毒/艾滋病预防支出从 5.96 亿美元(2.58 亿至 13 亿美元)增加到 30 亿美元(15 亿至 58 亿美元),艾滋病毒/艾滋病护理和治疗支出从 11 亿美元(4581 万至 220 亿美元)增加到 72 亿美元(43 亿至 118 亿美元)。在此期间,发展援助来源的资源份额从 33.2%(21.3%至 45.0%)增加到 46.0%(34.2%至 57.0%)。各国每年接受抗逆转录病毒疗法的护理和治疗支出各不相同,智商区间为 284 美元至 2915 美元。中低收入国家(阿根廷、中国、哥伦比亚、印度、印度尼西亚、墨西哥、尼日利亚、俄罗斯、南非和越南)的政府可以调动 121 亿美元(84 亿至 175 亿美元)的额外资金用于抗击艾滋病毒/艾滋病。这些潜在资源中的大部分集中在 10 个中等收入国家(阿根廷、中国、哥伦比亚、印度、印度尼西亚、墨西哥、尼日利亚、俄罗斯、南非和越南)。
一些政府可以调动更多的国内资源来对抗艾滋病毒/艾滋病,这可以为许多没有这种能力的国家释放更多的发展援助,包括许多低收入、高流行率的国家。然而,现有的资金与实现全球艾滋病毒/艾滋病目标所需的资金之间存在很大差距,需要国际和国内发展伙伴之间持续和协调的努力,才能在 2030 年之前结束艾滋病。
比尔及梅琳达·盖茨基金会。