Division of Cancer Medicine, Department of Stem Cell Transplantation, The University of Texas MD Anderson Cancer Center, Houston, TX.
University of Minnesota, Minneapolis, MN.
Blood Adv. 2019 May 14;3(9):1441-1449. doi: 10.1182/bloodadvances.2018030171.
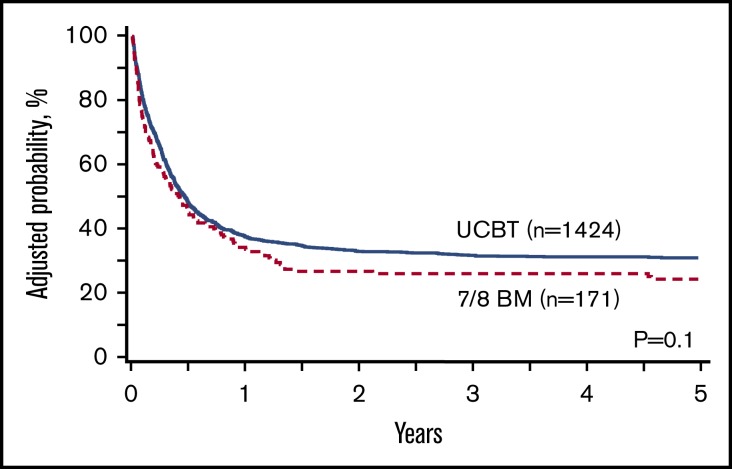
We report graft-versus-host disease (GVHD)-free relapse-free survival (GRFS) (a composite end point of survival without grade III-IV acute GVHD [aGVHD], systemic therapy-requiring chronic GVHD [cGVHD], or relapse) and cGVHD-free relapse-free survival (CRFS) among pediatric patients with acute leukemia (n = 1613) who underwent transplantation with 1 antigen-mismatched (7/8) bone marrow (BM; n = 172) or umbilical cord blood (UCB; n = 1441). Multivariate analysis was performed using Cox proportional hazards models. To account for multiple testing, < .01 for the donor/graft variable was considered statistically significant. Clinical characteristics were similar between UCB and 7/8 BM recipients, because most had acute lymphoblastic leukemia (62%), 64% received total body irradiation-based conditioning, and 60% received anti-thymocyte globulin or alemtuzumab. Methotrexate-based GVHD prophylaxis was more common with 7/8 BM (79%) than with UCB (15%), in which mycophenolate mofetil was commonly used. The univariate estimates of GRFS and CRFS were 22% (95% confidence interval [CI], 16-29) and 27% (95% CI, 20-34), respectively, with 7/8 BM and 33% (95% CI, 31-36) and 38% (95% CI, 35-40), respectively, with UCB ( < .001). In multivariate analysis, 7/8 BM vs UCB had similar GRFS (hazard ratio [HR], 1.12; 95% CI, 0.87-1.45; = .39), CRFS (HR, 1.06; 95% CI, 0.82-1.38; = .66), overall survival (HR, 1.07; 95% CI, 0.80-1.44; = .66), and relapse (HR, 1.44; 95% CI, 1.03-2.02; = .03). However, the 7/8 BM group had a significantly higher risk for grade III-IV aGVHD (HR, 1.70; 95% CI, 1.16-2.48; = .006) compared with the UCB group. UCB and 7/8 BM groups had similar outcomes, as measured by GRFS and CRFS. However, given the higher risk for grade III-IV aGVHD, UCB might be preferred for patients lacking matched donors.
我们报告了在接受 1 个抗原不匹配(7/8)骨髓(BM;n=172)或脐带血(UCB;n=1441)移植的儿童急性白血病患者(n=1613)中,无 III-IV 级急性移植物抗宿主病(aGVHD)[aGVHD]、需要系统治疗的慢性 GVHD(cGVHD)或复发的移植物抗宿主病-无复发存活率(GRFS)(无 III-IV 级 aGVHD、需要系统治疗的 cGVHD 或复发的生存的复合终点)和无 cGVHD 复发存活率(CRFS)。采用 Cox 比例风险模型进行多变量分析。为了进行多次检验,<.01 的供体/移植物变量被认为具有统计学意义。UCB 和 7/8 BM 受者的临床特征相似,因为大多数患者患有急性淋巴细胞白血病(62%),64%接受基于全身照射的预处理,60%接受抗胸腺细胞球蛋白或阿仑单抗。与 UCB(15%)相比,7/8 BM 中更常见甲氨蝶呤为基础的 GVHD 预防(79%),其中更常使用霉酚酸酯。7/8 BM 和 UCB 的单变量 GRFS 和 CRFS 估计值分别为 22%(95%置信区间[CI],16-29)和 27%(95% CI,20-34),分别为 33%(95% CI,31-36)和 38%(95% CI,35-40),分别为 7/8 BM 和 UCB(<.001)。在多变量分析中,7/8 BM 与 UCB 的 GRFS 相似(风险比[HR],1.12;95%CI,0.87-1.45; =.39)、CRFS(HR,1.06;95%CI,0.82-1.38; =.66)、总生存(HR,1.07;95%CI,0.80-1.44; =.66)和复发(HR,1.44;95%CI,1.03-2.02; =.03)。然而,与 UCB 组相比,7/8 BM 组 III-IV 级 aGVHD 的风险显著更高(HR,1.70;95%CI,1.16-2.48; =.006)。UCB 和 7/8 BM 组的 GRFS 和 CRFS 结果相似。然而,鉴于 III-IV 级 aGVHD 的风险较高,对于缺乏匹配供体的患者,UCB 可能是首选。