Department of Internal Medicine, University Medical Center Groningen, University of Groningen, 9713 GZ Groningen, The Netherlands.
Institute of Toxicology, Core Unit Proteomics, Hannover Medical School, Carl-Neuberg-Str. 1, 30625 Hannover, Germany.
Nutrients. 2019 May 10;11(5):1044. doi: 10.3390/nu11051044.
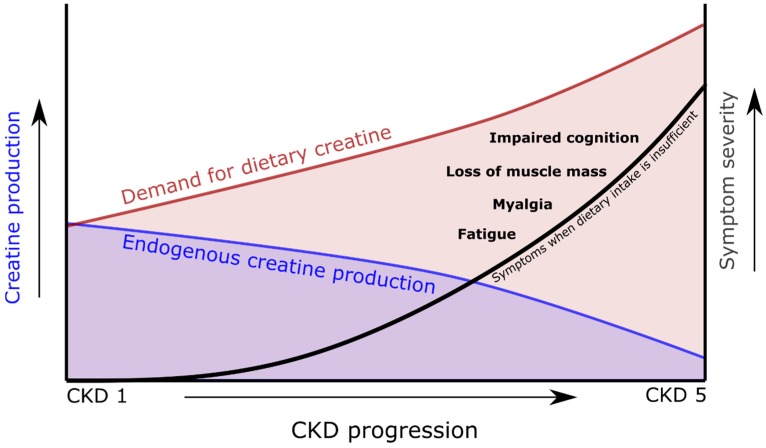
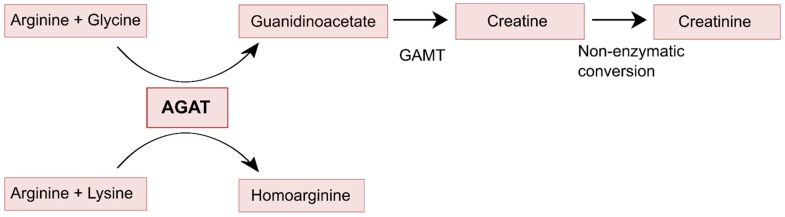
To accommodate the loss of the plethora of functions of the kidneys, patients with chronic kidney disease require many dietary adjustments, including restrictions on the intake of protein, phosphorus, sodium and potassium. Plant-based foods are increasingly recommended as these foods contain smaller amounts of saturated fatty acids, protein and absorbable phosphorus than meat, generate less acid and are rich in fibers, polyunsaturated fatty acids, magnesium and potassium. Unfortunately, these dietary recommendations cannot prevent the occurrence of many symptoms, which typically include fatigue, impaired cognition, myalgia, muscle weakness, and muscle wasting. One threat coming with the recommendation of low-protein diets in patients with non-dialysis-dependent chronic kidney disease (CKD) and with high-protein diets in patients with dialysis-dependent CKD, particularly with current recommendations towards proteins coming from plant-based sources, is that of creatine deficiency. Creatine is an essential contributor in cellular energy homeostasis, yet on a daily basis 1.6-1.7% of the total creatine pool is degraded. As the average omnivorous diet cannot fully compensate for these losses, the endogenous synthesis of creatine is required for continuous replenishment. Endogenous creatine synthesis involves two enzymatic steps, of which the first step is a metabolic function of the kidney facilitated by the enzyme arginine:glycine amidinotransferase (AGAT). Recent findings strongly suggest that the capacity of renal AGAT, and thus endogenous creatine production, progressively decreases with the increasing degree of CKD, to become absent or virtually absent in dialysis patients. We hypothesize that with increasing degree of CKD, creatine coming from meat and dairy in food increasingly becomes an essential nutrient. This phenomenon will likely be present in patients with CKD stages 3, 4 and 5, but will likely be most pronouncedly present in patients with dialysis-dependent CKD, because of the combination of lowest endogenous production of creatine and unopposed losses of creatine into the dialysate. It is likely that these increased demands for dietary creatine are not sufficiently met. The result of which, may be a creatine deficiency with important contributions to the sarcopenia, fatigue, impaired quality of life, impaired cognition, and premature mortality seen in CKD.
为了适应肾脏大量功能丧失,慢性肾脏病患者需要进行许多饮食调整,包括限制蛋白质、磷、钠和钾的摄入。植物性食物越来越受到推荐,因为这些食物中饱和脂肪酸、蛋白质和可吸收磷的含量低于肉类,产生的酸较少,并且富含纤维、多不饱和脂肪酸、镁和钾。不幸的是,这些饮食建议并不能预防许多症状的发生,这些症状通常包括疲劳、认知障碍、肌痛、肌肉无力和肌肉萎缩。在非透析依赖型慢性肾脏病(CKD)患者中推荐低蛋白饮食和透析依赖型 CKD 患者中推荐高蛋白饮食的同时,尤其是当前推荐来自植物性来源的蛋白质时,存在着肌酸缺乏的威胁。肌酸是细胞能量平衡的重要贡献者,但在日常情况下,总肌酸池的 1.6-1.7%会被降解。由于普通杂食性饮食不能完全弥补这些损失,因此需要内源性肌酸合成来持续补充。内源性肌酸合成涉及两个酶促步骤,其中第一步是肾脏的酶精氨酸:甘氨酸酰胺转移酶(AGAT)促进的代谢功能。最近的研究结果强烈表明,随着 CKD 程度的增加,肾脏 AGAT 的能力(即内源性肌酸的产生)逐渐降低,在透析患者中消失或几乎消失。我们假设,随着 CKD 程度的增加,食物中的肌酸越来越成为肉类和奶制品等必需营养素。这种现象可能存在于 CKD 3、4 和 5 期患者中,但在透析依赖型 CKD 患者中可能最为明显,因为内源性肌酸生成最低,同时肌酸无对抗地损失到透析液中。很可能这些对膳食肌酸的需求增加没有得到充分满足。其结果可能是肌酸缺乏,这对 CKD 患者中看到的肌肉减少症、疲劳、生活质量下降、认知障碍和过早死亡有重要贡献。